No one wants to pay for genetic medicines, especially gene editing therapies. This is a painful truth that patient advocates and startup founders alike have to face.
For years, leaders, even pioneers of CRISPR gene editing technologies, have passionately pleaded with government, banks, and the pharmaceutical industry for support. It only gets harder to hear when patients and their families are begging and praying, their fates blown one way or another by the actions of massive entities that shape the development, funding, and regulation of these potentially life-saving drugs. On the patient side, parents have been on the fence about research-as-care gene editing therapies because of the (rightly) perceived cost, millions of dollars.
Most gene-editing medicines target tiny patient populations, often numbering in the thousands worldwide, and can cost millions of dollars per patient. Manufacturing and delivery are far from solved. And despite years of excitement around CRISPR and related technologies, gene editing has yet to reshape mainstream medicine.
So, most parents don’t even get to choose whether to sell their house to save their child—they just watch and wait. For the thousands of monogenic inherited diseases, gene editing is a mirage, seemingly forming on the horizon only for it to vanish when reached.
That the rate-limiting factor is not in the science is clear as day. For nearly a decade, gene editing has carried the aura of scientific revolution while remaining, in practical terms, a niche corner of medicine. But the economics and scale of those therapies have remained limited.
Pharma behemoth Lilly appears to have picked up an ax, struck into this frozen wall, and made a sizeable crack with their experimental in vivo base-editing therapy VERVE-102. Originally developed by Verve Therapeutics, a recent Lilly acquisition, VERVE-102 is designed to permanently reduce cholesterol by switching off the PCSK9 gene inside liver cells. In adults with atherosclerotic cardiovascular disease (ASCVD), one dose of VERVE-102 should reduce PCSK9 and LDL-C levels safely, significantly, and sustainably.
Early clinical results, published in the New England Journal of Medicine, from 35 participants with heterozygous familial hypercholesterolemia (HeFH) or premature coronary artery disease (CAD) showed just that. This ongoing Heart-2 Phase Ib study could lead to the approval of a one-time, possibly best-in-class treatment for a condition that is a leading cause of death of adults worldwide. If ultimately validated, VERVE-102 could reshape cardiovascular medicine.
The trial is also one of the clearest signs that the biotech industry is progressing in transforming gene editing from a boutique technology for rare disease into a scalable platform for chronic illness.
Gene-editing wizard and base editor inventor David Liu, PhD, told Inside Precision Medicine, “I consider VERVE-102 to be important in several ways—as the first example of clinical in vivo base editing (note that now the majority of the 23+ clinical trials that use base or prime editing are in vivo!); as an effective, one-time treatment for a serious genetic disease (FH); and as a key demonstration of the use of precision gene editing for disease PREVENTION, not just for the correction of pathogenic mutations. In this case, lowering LDL reduces the risk of the #1 killer of humans around the world, so the potential implications of using precision gene editing to lower disease risk are vast.”
Uli Stilz, PhD, senior advisor at Flagship Pioneering, board member to biotech companies and venture capital funds, and advocate for using genetic editing approaches to treat complex diseases, echoed Liu’s statements. “VERVE-102 is important not simply because of the clinical results, but because it continues to test a much larger hypothesis: can one-time genetic medicines become practical therapies for common chronic diseases?” Stilz told Inside Precision Medicine. “The field is moving beyond proof of concept. The next challenge is demonstrating the combination of safety, durability, scalability, and clinical utility required for broad patient populations. If successful, this could represent a fundamental shift in how we think about the prevention and treatment of cardiovascular disease.”
Cutting off cholesterol at the genetic source
Two significant events from ten years ago underpinned the VERVE-102 results released this week. In April 2016, Alexis Komor, PhD, and Liu published the first base editor— programmable editing of a genomic DNA target base without double-stranded DNA cleavage— in Nature, rocking the gene editing world. The other, the idea behind Verve Therapeutics, was kept under wraps and thus did not cause nearly as much of a stir.
From its conception to its official founding in 2018, Verve Therapeutics co-founders Sekar Kathiresan, MD, and Kiran Musunuru, MD, PhD, anticipated that delivering gene-editing therapies safely into the body would be its biggest challenge. Kathiresan and Musunuru, one half of the clinical duo at the heart of the baby KJ story, intentionally developed multiple product candidates with different lipid nanoparticle (LNP) delivery systems to reduce that risk.
This approach became particularly important after Verve halted its Heart-1 trial of VERVE-101 in April 2024 due to a severe but reversible adverse event in one patient, which Verve attributed to the LNP delivery shell rather than the gene-editing machinery itself. While VERVE-101 used an Acuitas-developed LNP, Verve’s newer candidates, VERVE-102 and VERVE-201, rely on a second-generation GalNAc-enhanced LNP designed to improve both safety and targeting efficiency.
Despite the trial setback and stock decline, Verve showed the first human proof of concept for in vivo base editing, with permanent PCSK9 gene editing reducing LDL-C in early patients. A bit over a year later, in June 2025, Lilly made a prophetic acquiring Verve for north of $1 billion in all-cash. About two years after VERVE-101 and the Heart-1 trial were paused, VERVE-102’s historic results were announced and published.
In the interim Heart-2 analysis, Verve researchers treated 35 participants with HeFH or premature CAD across six escalating dose cohorts ranging from 0.3 mg/kg to 1.0 mg/kg. The results showed clear dose-dependent effects: mean reductions in circulating PCSK9 protein ranged from 51% at the lowest dose to 88% at the highest, and LDL-C reductions ranged from 9% to 62%, with participants in the highest-dose group seeing an average absolute LDL reduction of 78 mg/dL. Perhaps most striking was VERVE-102’s durability. Some participants have now been followed for up to 18 months, and cholesterol lowering has thus far persisted throughout follow-up.
Marc S. Sabatine, MD, chairman of the Thrombolysis in Myocardial Infarction (TIMI) Study Group, Endowed Chair in Cardiovascular Medicine at Brigham and Women’s Hospital (BWH), and professor of medicine at Harvard, put the efficacy findings into context with existing cardiovascular medications. In speaking with Inside Precision Medicine, Sabatine said, “The reductions in LDL-C are on par with what has been seen for the monoclonal antibody PCSK9 inhibitors and, more recently, the oral PCSK9 inhibitor enlicitide. Moreover, the effect appears durable, with data out to one year.”
Researchers reported no dose-limiting toxicities. The most common side effects reported from the Heart-2 trial were mild-to-moderate infusion-related reactions and temporary elevations in liver enzymes. One participant developed aspiration pneumonitis associated with pre-existing gastroesophageal reflux disease.
According to Lilly, with no unanticipated safety findings observed, the overall safety profile remains encouraging. Sabatine added, “In this small number of patients, the safety profile appears good so far, with only mild to moderate infusion reactions and only transient, mild elevations in levels of aminotransferases.”
All of the participants are expected to enroll in a long-term follow-up study for up to 15 years. The long-term follow-up requirement reflects both the promise and the tension of permanent gene editing. Unlike conventional drugs, DNA edits may persist for decades—potentially for life. That raises the possibility of lifelong benefit from a single treatment but also creates unusually high regulatory scrutiny around safety and durability.
“These data, although very preliminary, are exciting,” Sabatine said. “If these observations are confirmed in larger and longer studies, VERVE-102 would be another powerful tool in our PCSK9 inhibitor armamentarium, which might someday allow patients to choose between a daily pill, periodic injections, or a once-in-a-lifetime infusion.”
According to a Lilly spokesperson, enrollment in the Heart-2 study is ongoing, together with continued participant follow-up. Together with the safety findings, these data will help inform dose selection for Phase II of the study, which is expected to begin before year-end.
Lilly isn’t the only horse in the race, which began to heat up in March 2026 when Chinese researchers published a study in Nature using their own in vivo PCSK9 base editor delivered via GalNAc-modified LNPs YOLT-101 to patients with HeFH. In a Phase I study with Shanghai Jiao Tong University School of Medicine and the Shanghai Key Laboratory of Precision Gene Editing and Clinical Translation, YolTech Therapeutics reported that YOLT-101 reduced LDL-C by 52.3% and circulating PCSK9 protein by 74.4% at 24 weeks in patients receiving the highest dose.
Lilly’s bet on scale
Lilly appears to be making a calculated bet that gene editing can evolve into a commercially viable platform for chronic disease—not just scientifically, but economically. That would represent a dramatic shift for the field. Rare disease therapies often justify high prices because they target extremely small patient populations. But cardiovascular disease operates on an entirely different scale. Elevated LDL-C affects hundreds of millions of people worldwide. Even a fraction of that market would dwarf nearly every current gene therapy indication.
The challenge is that gene-editing medicines have historically struggled with scalability, manufacturing costs, and delivery efficiency. To succeed commercially in chronic disease, companies will likely need therapies that are easier to manufacture, simpler to administer, safer in broader populations, and capable of producing durable benefit from a single intervention.
At the same time, Lilly is positioning genetic medicine not as a niche business unit but as a central long-term pillar of the company’s research strategy. According to Lilly, VERVE-102 is a key part of Lilly’s growing genetic medicines portfolio, which now accounts for more than one-third of the company’s R&D portfolio.
Since the Verve acquisition, Lilly has made several acquisitions that echo Kathiresan and Musunuru’s concern with genetic medicine delivery. The acquisitions of Kelonia Therapeutics and EngageBio expand Lilly’s genetic medicine capabilities with novel viral and non-viral in vivo gene delivery and integration technology, respectively, that has potential for broad applicability. Since these acquisitions are only applicable in oncology, Lilly will face a major challenge in expanding its targeting from the liver, the default homing site for many LNPs, to the rest of the body.
The company’s strategy reveals a broader industry transition now underway: using the massive profits generated by today’s blockbuster chronic-disease drugs to finance the development of entirely new therapeutic paradigms. Lilly’s current growth has heavily relied on incretin-based obesity and diabetes drugs, medicines that typically require continuous use. Gene editing, by contrast, could theoretically reduce or eliminate recurring treatment altogether. The Lilly spokesperson added, “Incretin-based therapies are transforming care for many people today, while genetic medicines represent a longer-term investment in approaches that could potentially shift some diseases from chronic management toward more durable intervention.”
These complementary approaches appear to be sufficient in making the risky and costly field of gene editing a strategic bet for Lilly. It may even be necessary. For pharmaceutical companies, that creates both a challenge and an opportunity: replacing recurring chronic revenue models with potentially curative interventions that may command large upfront prices but fewer repeat prescriptions.
Rare to population, reactive to prevention
The VERVE-102 data also highlight how rapidly genetic medicine is expanding beyond its original targets. “Genetic medicines have historically focused on rare diseases, and we believe they continue to hold significant potential for areas that have received less attention due to smaller patient populations and limited commercial incentives,” said a Lilly spokesperson. The company is exploring opportunities to apply these platforms across a range of conditions, “including inherited sensory disorders such as genetic hearing and vision loss, as well as chronic diseases where the underlying biology is well understood.”
What the early results from Heart-2 show is that gene-editing drugs need not only be reactive. Rather, if used preventively, drugs like VERVE-102 may ultimately prove the most disruptive aspect of gene editing in common disease. Lilly says that the early results from the Heart-2 study offer “an encouraging example of the potential in chronic diseases—treating disease at its source but also potentially shifting care from reactive treatment to earlier intervention and, in some cases, prevention.”
Historically, cardiovascular medicine has focused on lowering risk after damage has already begun accumulating. Patients develop plaque over decades, then receive progressively more intensive therapies as disease advances. A one-time gene-editing intervention administered earlier in life could theoretically alter that trajectory before severe disease develops.
Lilly and Verve researchers are already exploring adjacent approaches. In addition to the PCSK9 program, the Pulse-1 Phase Ib trial for VERVE-201 is testing another in vivo gene-editing therapy targeting ANGPTL3, another important regulator of lipid metabolism.
Together, the programs suggest a future in which cardiovascular disease may eventually be treated not with escalating layers of medication, but with molecular interventions designed to reset risk factors permanently at their genetic source. That future remains far from certain. Researchers still need to prove long-term safety, establish cardiovascular outcome benefits, and demonstrate that permanent editing can be deployed reliably across broad populations.
But the direction of the gene editing field is clearly no longer confined to the rarest diseases in medicine. And if therapies like VERVE-102 ultimately succeed, the age of in vivo gene editing may no longer be defined by rare disease at all, but by the much larger ambition of rewriting the treatment model for chronic illness itself.
Revolution Medicines reports that its investigational drug daraxonrasib doubled the overall survival of patients with metastatic pancreatic cancer compared to standard chemotherapy, according to results from the Phase III RASolute 302 trial. These findings were published yesterday in The New England Journal of Medicine and presented at the 2026 American Society of Clinical Oncology (ASCO) Annual Meeting.
“In this trial, daraxonrasib redefined treatment expectations in previously treated metastatic pancreatic cancer by reducing the risk of death by 60% and increasing median overall survival to more than one year, a result not previously reported in any Phase III clinical trial in any line of therapy for this disease,” said Mark A. Goldsmith, MD, PhD, chief executive officer and chairman of Revolution Medicines.
Pancreatic ductal adenocarcinoma (PDAC) is one of the deadliest cancer diagnoses, with a five-year survival rate of 3%. Currently available therapies offer very limited benefits for these patients, especially for those who have already been treated with a first line of chemotherapy and continued to see tumor progression.
In over 90% of pancreatic tumors, mutations that result in an overactivation of RAS(ON) signaling are a major driver of cancer growth. Daraxonrasib is an oral drug designed to block a broad spectrum of wild type and mutant RAS variants. The RASolute 302 trial set out to compare the effects of a daily dose of daraxonrasib to a standard chemotherapy course in 500 patients with metastatic pancreatic cancer who had previously received a first line of chemotherapy.
Results show that daraxonrasib increased the median overall survival from 6.6 to 13.2 months, while boosting progression-free survival from 3.5 to 7.3 months. Notably, these effects were consistent regardless of whether the tumors carried RAS mutations. Serious side effects were reported less frequently by patients who received daraxonrasib, reducing the likelihood of a patient having to discontinue treatment due to side effects by 10 times.
“Daraxonrasib significantly elevates the survival bar in the treatment of one of the deadliest human cancers, while better preserving quality of life compared to chemotherapy,” said Goldsmith. “These striking results firmly support daraxonrasib as the new standard of care for patients with previously treated metastatic pancreatic cancer, and usher in a new era of RAS-targeted therapy for patients living with this disease.”
Revolution Medicines has stated its intention to submit this data to the FDA and other regulators to seek approval of daraxonrasib in this patient population. Three other Phase III trials are currently underway, evaluating the drug in patients with PDAC and metastatic non-small cell lung cancer.
“These results from the Phase III RASolute 302 trial of daraxonrasib represent a major milestone for patients facing metastatic pancreatic cancer,” said Brian M. Wolpin, MD, director of the Hale Family Center for Pancreatic Cancer Research at the Dana-Farber Cancer Institute, professor of medicine at Harvard Medical School, and principal investigator for the RASolute 302 trial.
“For many patients, second line chemotherapy provides modest benefits, and new treatments delivering more durable tumor control have been urgently needed. These results will change how scientists, clinicians, and patients think about treatment for pancreatic cancer, and support a new paradigm where RAS(ON) inhibition enters standard of care for patients with previously treated metastatic pancreatic adenocarcinoma.”
Some of the forces that shape biopharma cluster development are constants year after year, such as the emergence of startups from university and research institute labs to develop new treatments, thanks to ideas backed by the brains of researchers and executives, and the bucks of serial entrepreneurs and other investors.
But in recent years, several additional unique circumstances have come to reshape how much and especially where biopharmas choose to grow, Matthew Gardner, CBRE Americas Life Sciences Leader, shared with GEN recently.
One is increased acquisition of lab and manufacturing properties by “mid-cap” biopharmas ranging between $2 billion and $10 billion in market capitalization (share price times the number of outstanding shares), as they seek to better control their supply chains by maintaining their own infrastructure in evolving from research- to commercialization-focused drug developers.
“They might have been more likely to lease in a different circumstance. They’ve definitely caught an opportunity to jump in and take ownership. That has been an ongoing trend, and that has been true coast-to-coast in most of the major centers,” Gardner said.
Among investor-owners, Gardner said, another transition has begun from pure-play biopharma real estate landlords to investors with broader portfolios encompassing healthcare—a reflection of how the two fields are increasingly converging. During December 2025 and January 2026, for example, the public real estate investment trust (REIT) Healthpeak shelled out $600 million to close on the acquisition of a 1.4-million square foot, 29-acre campus on Gateway Boulevard in South San Francisco, CA, from the nation’s largest biopharma REIT, Alexandria Real Estate Equities and BXP (formerly Boston Properties).
Those and other investors aim to cash in on the improving climate for biopharmas seeking to raise capital, from a recovering venture capital market to increased merger-and-acquisition (M&A) activity, and, in recent weeks, a revived market for initial public offerings (IPO).
Another key factor in recent cluster-building cited by Gardner is the “reshoring” of manufacturing in the U.S. by global biopharma giants, whether to satisfy growing demand for treatments—especially obesity drugs—or avoid tariffs, or both. While many of those new facilities are in manufacturing-heavy clusters like North Carolina and Greater Philadelphia, others have spread into Maryland and Virginia (the BioHealth Capital Region), and several new biomanufacturing sites have been built or are under construction in emerging clusters outside the Top 10—a trend GEN plans to explore in the coming weeks.
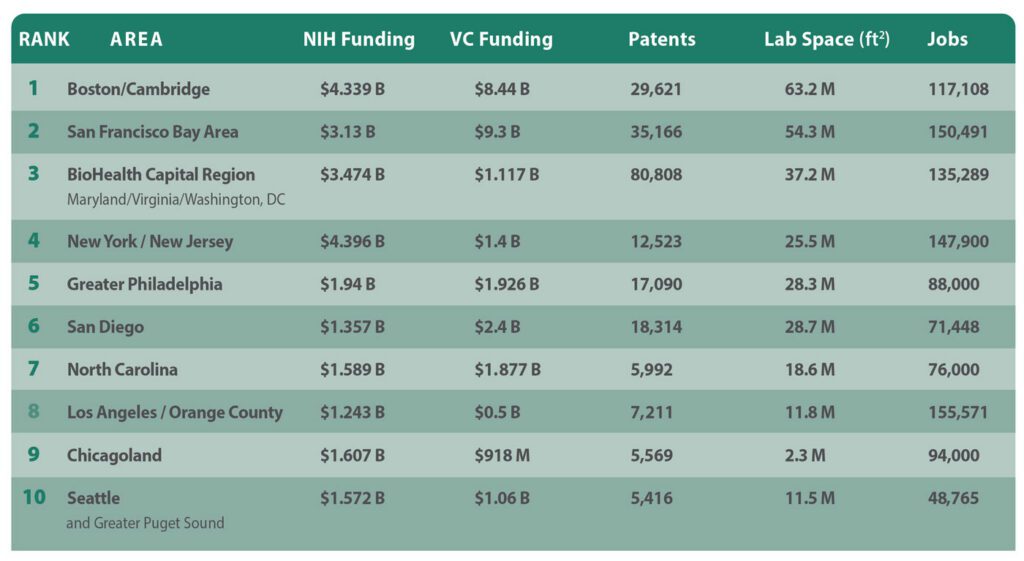
Speaking of top 10 clusters, GEN presents its latest edition of its nationally- and regionally-cited annual A-List of its top 10 U.S. biopharma cluster rankings, designed to show which regions are most competitive in attracting life sciences leaders, companies, and institutions. Over more than a decade, GEN has based its rankings on five criteria:
Patents: Figures from the Patent Public Search database of the U.S. Patent and Trademark Office, showing the number of patent families containing the word “biotechnology” and towns and cities within a given region or state.
NIH funding: Figures for NIH funding were taken from the publicly available NIH Research Portfolio Online Reporting Tools (RePORT) database for the current federal fiscal year through May 4, plus all of fiscal year 2025 (October 1, 2024, through September 30, 2025).
Venture capital funding: Figures for all of 2025 and the first quarter of 2026 as compiled by regional life sciences groups and PitchBook, which joins with the National Venture Capital Association to publish the quarterly Venture Monitor reports.
Laboratory space: The total-size-of-market figure, in millions of square feet, as furnished by regional life sciences groups. In regions that did not compile such information, the figure cited is the highest by any of several commercial real estate companies, including CBRE Group, Colliers, Cushman & Wakefield, JLL, and Newmark.
Number of jobs: The preferred sources for job figures were regional life sciences groups. Alternative sources included commercial real estate firms.
1. Boston/Cambridge, MA
Genentech has agreed to more than triple its space, growing from 30,000 to 100,000 square feet, within 1 Milestone Street at the Harvard University-owned, Tishman Speyer-developed Enterprise Research Campus in Boston’s Allston section [Breakthrough Properties, Studio Gang & Henning Larsen]
Years of growing into the nation’s top biopharma cluster have taken a toll on Boston and adjacent Cambridge, MA: The Wall Street Journal in December highlighted the inability of Boston-area PhDs to find work, while the region faces a glut of life sciences space as biopharmas and real estate developers scale back earlier plans—a 32.7% availability rate according to CBRE, up 70 basis points from Q1 2025. Takeda Pharmaceutical in March eliminated 247 jobs in Massachusetts, where the company has facilities in Lexington, MA, and Cambridge, part of a $1.3 billion restructuring that cut 634 jobs nationwide. Replimune in April chopped 223 jobs at its Woburn, MA, HQ, and Framingham, MA, manufacturing site after the FDA rejected its BLA seeking approval for RP1 [plus Bristol Myers Squibb’s Opdivo® (nivolumab)] for advanced melanoma. In February, Takeda placed 449,140 square feet within three Cambridge buildings on the sublease market, a week after Alexandria Real Estate Equities scrapped plans to convert 401 Park Drive in Boston’s Fenway section into lab space, with CEO and chief investment officer Peter M. Moglia saying the real estate investment trust was pivoting to meet growing demand for office space.
Among the region’s growing life-science companies: Genentech agreed to more than triple its space, growing from 30,000 to 100,000 square feet within One Milestone Street at the Harvard University-owned, Tishman Speyer-developed Enterprise Research Campus in Boston’s Allston section. Hemab Therapeutics (based in Cambridge and Copenhagen) and Seaport Therapeutics (Boston) both priced IPOs on April 30, raising $301.5 million and $254.88 million, respectively—a day after Avalyn Pharma (Boston) garnered $300 million in its IPO. In March, Terrestrial Bio became the first life-science tenant at Allston Labworks (250 Western Avenue) by leasing 42,000 square feet at the mixed-use building within Boston’s Allston neighborhood, while AI Proteins in January inked a 40,000-square-foot lease at 660 Commonwealth Avenue, within Related Beal’s One Kenmore Square in Boston. Regional companies finding buyers in April include Boston-based Kelonia Therapeutics and Cambridge-based Ajax Therapeutics, both to be acquired by Eli Lilly (for up to $7 billion and up to $2.3 billion, respectively) and Framingham-based KalVista Pharmaceuticals, to be acquired by Italy’s Chiesi Group for about $1.9 billion.
Boston/Cambridge enjoys the nation’s largest portfolio of lab space (63.2 million square feet according to industry group MassBio), but was bested by the San Francisco Bay Area in NIH funding (7,037 awards totaling $4.339 billion) following a year of government funding cuts. The region also placed second in VC ($6.85 billion in 2025, says MassBio; $1.59 billion in Q1 2026, according to PitchBook data cited by MassBio), but landed third in patents (29,621 families) and just fifth in jobs (117,108, according to MassBio).
2. San Francisco Bay Area
Eli Lilly Chair and CEO David A. Ricks and Nvidia Founder, president, and CEO Jensen Huang announce the companies’ five-year, $1 billion partnership to create a “Co-Innovation AI Lab” designed to address key challenges in AI drug discovery, announced on January 12 during the J.P. Morgan 44th Annual Healthcare Conference in San Francisco. The lab will be located within the Bay Area. [Nvidia]
Santa Clara, CA-based Nvidia and Eli Lilly electrified the annual J.P. Morgan Healthcare Conference, held in downtown San Francisco each January, by announcing a five-year, $1-billion collaboration to create a “Co-Innovation AI Lab” in the region to address key challenges in artificial intelligence (AI) drug discovery, powered by a supercomputer that went live in February. That welcome news aside, more than one-third of the region’s life-science space is available for lease (33.7% as of Q1, according to CBRE). And more space has entered the market: Pfizer confirmed plans in April to shut down its 164,000-square-foot research facility at 181 Oyster Point Blvd. in South San Francisco, CA, shifting employees to remote jobs. Cushman & Wakefield is marketing the space for sublease. Also, on the market in “South City” is a 21,552-square-foot lab building and surrounding 3.65 acres previously occupied by the U.S. Department of Agriculture, which is selling the building for just under $48 million. In May, Foster City, CA-based Gilead Sciences disclosed plans to lay off 108 employees based in Redwood City, CA, (and 84 in Rockville, MD) following its $7.8-billion acquisition of Arcellx.
Not all the recent news is bad: Gladstone Institutes plans early next year to open approximately 20 new labs employing about 300 scientists within the 105,000 square feet it agreed to lease in March at 1450 Owens Street, within Alexandria Real Estate Equities’ Alexandria Center® for Science and Technology–Mission Bay Megacampus. Natera inked a 62,969-square-foot lease at Brittan West in San Carlos, CA, in February. And last fall, Elon Musk’s Neuralink leased the entire approximately 144,000-square-foot 499 Forbes Boulevard in South San Francisco. On the financing side, SF-based Breakout Ventures in March closed its $114-million Fund III, which aims to invest in founder-led companies applying AI in biopharma, while Palo Alto, CA-based Surf Bio, whose lead investor for its only institutional round was Breakout, was acquired by San Diego-based Halozyme Therapeutics for up to $400 million, in a deal announced in January.
San Francisco and its suburbs topped Boston/Cambridge in VC ($7.8 billion in 2025, $1.5 billion in Q1 2026, both according to PitchBook). The Bay Area is second in three criteria: patents (35,166 families), lab space (54.3 million square feet according to Colliers), and jobs (150,491 according to BIOCOM California, but “more than 147,000” according to CBRE, both from last year). In NIH funding, the region is fourth (5,180 awards totaling $3.13 billion).
3. BioHealth Capital Region (Maryland, Virginia, and Washington, D.C.)
AstraZeneca has expanded the scope of its new manufacturing facility in Rivanna Futures, near Charlottesville, VA, into a $4.5 billion project designed to support manufacturing for weight management, metabolic, and cancer technologies, including antibody-drug conjugates. The project is expected to create 600 permanent jobs. [AstraZeneca]
The BHCR takes in Virginia and Maryland, both of which benefited over the past year from the domestic “reshoring” of biomanufacturing by pharma giants. AstraZeneca in November announced $2 billion in plans for Maryland that include a major expansion of its biologics manufacturing facility in Frederick, MD, and a new clinical manufacturing facility in Gaithersburg, MD. A month earlier, AstraZeneca expanded the scope of its new manufacturing facility in Rivanna Futures, near Charlottesville, VA, into a $4.5-billion project designed to support manufacturing for weight management, metabolic, and cancer technologies, including antibody-drug conjugates. The project is expected to create 600 permanent jobs. Also last fall, Merck & Co. broke ground on a $3 billion, 400,000-square-foot Center of Excellence for Pharmaceutical Manufacturing at its longstanding site in Elkton, VA, while Eli Lilly announced plans for a $5-billion manufacturing facility just west of Richmond, VA, in Goochland County that will be the company’s first-ever dedicated, fully integrated active pharmaceutical ingredient (API) and drug product facility for its bioconjugate platform and monoclonal antibody portfolio. However, a longtime strength of the region—the headquarters presence of the NIH and FDA—is now among its most serious challenges as government funding cuts chopped the workforces of both agencies last year by 3,500 and 1,200 jobs, respectively, though the FDA in recent months has worked to hire 1,000+ new staffers to fill reviewer, inspector, and investigator roles. And in May, Gilead Sciences disclosed plans to lay off 84 employees in Rockville, MD (and 108 in Redwood City, CA) following its $7.8-billion acquisition of Arcellx.
The BioHealth Capital Region fulfills its top-three cluster ambitions by continuing to lead the nation in patents (80,808 families) while placing third in NIH funding (4,665 awards totaling $3.474 billion) and lab space (37.208 million square feet according to JLL data cited by BHCR, including 9.2 million square feet of NIH labs in Bethesda, MD). The region is fourth in jobs (135,298, according to JLL and state data cited by BHCR), but seventh in venture capital ($1.117 billion in 2025, zero in Q1 2026, according to BHCR data).
4. New York/New Jersey
In New Jersey, New Brunswick’s Planning Board in February approved the $468 million H-3, the third phase of the HELIX downtown campus, a 40-story 554,000 square foot tower, for which the city council approved a 30-year PILOT agreement that will generate $1.8 million a year in annual payments in lieu of taxes [DEVCO New Brunswick Development Corp.]
The Big Apple will soon see a big biotech campus emerge, the $1.6 billion, 2-million-plus-square-foot Science Park and Research Campus (SPARC) Kips Bay, projected to create more than 15,000 jobs by combining life-science space with academic and public health facilities. Exterior demolition is scheduled for the third quarter, followed by construction next year. However, Johnson & Johnson has shifted operations of its JLABS@NYC incubator to site owner New York Genome Center, part of a corporate cutback of its incubator network. The 17-member Emerging Technology Advisory Board appointed by New York Gov. Kathy Hochul (D), who is seeking re-election this year, proposed numerous efforts in December to expand life sciences activity statewide, including a $65-million “Excellence” fund and a $40-million pre-commercialization fund. At deadline, the fate of those efforts was unknown despite a tentative agreement on May 7 of a $268-billion state budget.
In New Jersey, New Brunswick’s Planning Board in February approved the $468-million H-3, the third phase of the HELIX downtown campus, a 40-story, 554,000-square-foot tower, for which the city council approved a 30-year PILOT agreement that will generate $1.8 million a year in annual payments in lieu of taxes. In suburban Westchester County, Regeneron Pharmaceuticals is completing a $1.8-billion HQ expansion in Tarrytown but has scuttled earlier plans to expand across the Hudson River into the Rockland County village of Suffern, where the company spent $39 million to buy an old Avon Cosmetics warehouse for conversion into an infectious disease lab and a cold storage facility. In February, Regeneron hired JLL to market the site for sublease.
New York and its northern New Jersey suburbs lead the nation in NIH funding (7,033 awards totaling $4.396 billion) and are third in jobs (147,900, according to Cushman & Wakefield). From there, the region falls to the middle of the pack, placing fifth in VC ($1 billion in 2025 and about $400 million in Q1 2026, both according to PitchBook), and sixth in both lab space (25.5 million square feet, according to Colliers) and patents (12,523 families).
5. Greater Philadelphia
Eli Lilly made history in January by announcing Pennsylvania’s largest-ever biotech project, a $3.5 billion biomanufacturing site planned for Upper Macungie Township, an hour’s drive northwest of Philadelphia. Lilly plans to base 850 jobs at the plant, which will produce retatrutide and other weight loss drugs when it becomes operational in 2031. Lilly also has plans for Philadelphia, namely a 44,000-square-foot Lilly Gateway Labs innovation hub in Center City West at 2300 Market set to open later this year. [Eli Lilly]
Eli Lilly made history in January by announcing Pennsylvania’s largest-ever biotech project, a $3.5-billion biomanufacturing site planned for Upper Macungie Township, an hour’s drive northwest of Philadelphia. Lilly plans to base 850 jobs at the plant, which will produce retatrutide and other weight loss drugs when it becomes operational in 2031. Lilly also has plans for the City of Brotherly Love, namely a 44,000-square-foot Lilly Gateway Labs innovation hub in Center City West at 2300 Market set to open later this year. And, in Philadelphia’s Old City, Thermo Fisher Scientific last November opened its East Coast Advanced Therapies Collaboration Center (ATxCC) within the BioLabs for Advanced Therapeutics incubator.
Thermo Fisher Scientific executives last November celebrated the opening of the biotech tools giant’s East Coast Advanced Therapies Collaboration Center (ATxCC) in Philadelphia’s Old City, within the BioLabs for Advanced Therapeutics incubator. [Thermo Fisher Scientific]
The region’s rich biotech history includes the first gene therapy Luxturna® marketed by Roche-owned Spark Therapeutics—which is completing its $575 million Gene Therapy Innovation Center in University City despite laying off more than half of its Philly staff last year. In March, TerraPower Isotopes announced plans for a $450-million radioisotope manufacturing facility designed to produce actinium-225 for cancer treatments. The project will employ 225, receive $10 million in state grants, and rise within The Bellwether District, the 1,300-acre former Philadelphia Energy Solutions refinery site. Greater Philadelphia has long benefited from innovations from its institutions, two of which won more than $100 million in NIH funding during the 2025 federal fiscal year, the Perelman School of Medicine at the University of Pennsylvania to Children’s Hospital of Philadelphia (CHOP)—which last year treated KJ Muldoon (“Baby KJ”), the world’s first patient to receive a personalized CRISPR gene-editing therapy (for CPS1 deficiency). The region’s needs for more C-suite talent and venture capital remain persistent challenges to cluster growth, stakeholders told The Philadelphia Inquirer in December, though Audrey Greenberg, chair of corporate development and “Mayo Venture Partner” at Mayo Clinic and founder of AG Capital Advisors, told the Inquirer: “I’m going to be starting my companies all here in Philadelphia, because that’s where I am.”
Greater Philadelphia improved the most this year, climbing two positions in this year’s A-List after remaining fifth in patents (17,090 families) and rising to fifth in lab space (25.9 million square feet, according to Colliers’ data cited by Pennsylvania’s Department of Economic Development or DECD) and NIH funding (3,201 awards totaling $1.94 billion). The region jumped four spots to fifth in VC ($1.31 billion in 2025, $616 million in Q1 2026, says Colliers), but dipped to seventh in jobs (88,000, also according to DECD), including nearly 10,000 with cell and gene therapy expertise.
6. San Diego
Novartis broke ground in February on a $1.1 billion, 466,000-square-foot global Biomedical Research center in San Diego, expected to house 1,000 employees when operational in 2029, three months after opening a radioligand therapy manufacturing facility for cancer treatments in Carlsbad, CA. [Novartis]
The Biotechnology Innovation Organization (BIO) expects to draw 20,000 to its BIO International Convention when it returns this month to the San Diego Convention Center. The region remains a vibrant life-sciences cluster: Novartis broke ground in February on a $1.1-billion, 466,000-square-foot global Biomedical Research center in San Diego, expected to house 1,000 employees when operational in 2029, three months after opening a radioligand therapy manufacturing facility for cancer treatments in Carlsbad, CA. Eli Lilly in March completed its $1.2-billion acquisition of home-grown Ventyx Biosciences—months after the pharma opened a Lilly Gateway Labs innovation hub with Alexandria Real Estate Equities in Torrey Pines. The J. Craig Venter Institute—whose founder died April 29 at age 79—plans this summer to move its West Coast headquarters from the University of California San Diego campus in La Jolla to the downtown Research and Development District (RaDD), a $1.6-billion, 1.7-million-square-foot campus on the city’s Pacific coastline completed last year by San Diego-based developer IQHQ—which is fighting an investor’s fraud allegations related to a $50-million investment in 2020. Home-grown F5 Therapeutics (up to 10 employees) folded in March, while two other San Diego biotechs laid off employees this year: Gossamer Bio (65 employees, nearly half its workforce, as of May 15, following a Phase III trial failure) and BioAlta (70% of its staff, which was 41 as of December 31, 2025). In February, San Diego drug developer Iambic Therapeutics inked an up-to-$1.7-billion collaboration with Takeda Pharmaceutical, which will use Iambic’s AI technologies and wet lab capabilities to design and develop small molecule drugs. And global contract development and manufacturing organization (CDMO) Bora Biologics, in January, opened a $30-million expanded manufacturing facility with two to four 2,000-liter bioreactors, corresponding seed trains, and advanced downstream processing equipment.
“America’s Finest City” and vicinity stayed third in VC ($1.9 billion in 2025, says PitchBook, $743 million in Q1 2026 according to a GEN spot-check of recent deals) and fourth in patents (18,314 families) but dipped to fifth in lab space (28.685 million square feet, according to CBRE). While the San Diego region last year rose to ninth in NIH funding (2,001 awards totaling $1.357 billion), it slid to ninth in jobs (71,448, according to year-old BIOCOM California data).
7. North Carolina
Roche’s Genentech subsidiary in January expanded to $2 billion its planned investment in its first East Coast manufacturing facility in Holly Springs, NC, which broke ground last year and is set to support 500+ manufacturing jobs when operational by 2029. [Genentech]
Always strong on drug manufacturing, North Carolina is among the biggest beneficiaries of biopharma’s reshoring push. In April, AbbVie announced a $1.4-billion, 185-acre drug production facility in Durham County near Research Triangle Park (RTP), expected to employ 734. Roche’s Genentech subsidiary in January expanded to $2 billion its planned investment in its first East Coast manufacturing facility in Holly Springs, NC, which broke ground last year and is set to support 500+ manufacturing jobs when operational by 2029. And in November 2025, Novartis said it will expand Tar Heel State operations into a flagship manufacturing hub by adding capabilities for sterile filling of biologics into syringes and vials at its current Durham site, constructing two new Durham facilities for manufacturing biologics and sterile packaging, and building a new Morrisville, NC, site to produce solid dosage tablets and capsules, including packaging. Morrisville is where Novartis also plans to build a 56,200-square-foot facility focused on API manufacturing for solid dosage tablets, capsules, and RNA therapeutics, a project announced April 30. Manufacturing sites account for most of the combined $24.5 billion in new or expanded facilities with a potential 15,000+ new jobs that life sciences companies have announced statewide since 2021, according to the state-funded North Carolina Biotechnology Center. As for startups, Raleigh-based Slate Medicines launched in February with $130 million in Series A financing to fund development of therapies led by its migraine candidate, the anti-PACAP monoclonal antibody SLTE-1009 licensed from Zhongshan, China-based DartsBio Pharmaceuticals, and set to start Phase I trials in mid-2026.
The Tar Heel State climbed to fourth in VC ($1.6 billion in 2025, $276.8 million in Q1 2026, both according to the state-funded North Carolina Biotechnology Center). But North Carolina showed consistency on the other criteria, ranking seventh in NIH funding (2,248 awards totaling $1.589 billion) and lab space (18.6 million square feet, according to JLL), and eighth in jobs (76,000, says the Center) and patents (5,992 families).
8. Los Angeles / Orange County, CA
Amgen executives mark the groundbreaking for the biotech giant’s $600 million center for science and innovation being built within its Thousand Oaks, CA, headquarters campus, set to integrate Research & Development and Process Development teams to smoothen the transition from drug discovery to commercial manufacturing. [Amgen]
The region’s biopharma anchor Amgen broke ground last fall on a $600-million center for science and innovation being built within its Thousand Oaks, CA, headquarters campus, set to integrate research & development and process development teams to smooth the transition from drug discovery to commercial manufacturing. “With the first shovel in the ground, we’re reaffirming something essential: We discover here, we manufacture here, we deliver for patients from Thousand Oaks to all around the world,” Amgen chairman and CEO Robert A. Bradway said. Regional industry group BioscienceLA CEO Stephanie Hsieh recently acknowledged the region’s fragmentation as a challenge—from 88 cities in LA County alone, to the numerous county, city, and private agencies focused on growing the bioindustry— while citing strengths such as corporate anchors Amgen, Takeda Pharmaceutical, and Gilead Sciences-owned Kite Pharma, plus institutions like USC, UCLA, Cedars-Sinai, and City of Hope.
California signaled interest in growing the region’s biopharma industry last August when the state-funded California Jobs First Regional Investment Initiative awarded $23.92 million to a coalition led by Los Angeles County’s Department of Economic Opportunity (DEO) toward four programs intended to create 10,000 jobs by 2030. Most of the money ($19 million) was approved for a DEO revolving loan fund to support startups, especially those looking to graduate from the Larta Institute’s commercialization and capital access accelerator into lab space within Los Angeles County. Larta was awarded $3.3 million to expand its Heal.LA Bioscience & Healthcare Accelerator and assist small startups via its Larta Impact Fund, a revolving loan fund.
Los Angeles/ Orange County would still lead the nation in jobs, based on a year-old BIOCOM California tally of 155,571, which also includes San Bernardino and Ventura counties; figures run as low as 116,000, compiled last year for the four counties plus Riverside and Santa Barbara counties (regional industry group SoCalBio). The region finished seventh in patents (7,211 families), eighth in lab space (11.7 million square feet, according to JLL), and 10th in both NIH funding (1,911 awards totaling $1.243 billion) and VC ($500 million in 2025, zero in Q1 2026, according to PitchBook).
9. Chicagoland
AbbVie plans to build two new active pharmaceutical ingredient (API) manufacturing facilities totaling $380 million at its campus in North Chicago, IL, where the biopharma giant is headquartered. [AbbVie]
At least one developer has pivoted to a large non-biotech tenant to help fill a Chicago campus once envisioned as a life-sciences mecca: Trammell Crow in March inked a $100-million, 169,860-square-foot lease with candy/chocolate giant Mars to base 600 jobs at 400 North Aberdeen Street within the Fulton Market campus. Other biotech spaces are in the works: In North Chicago, Rosalind Franklin University of Medicine and Science plans to nearly double the size of its Helix 51 biomedical incubator to just under 13,000 square feet by adding 6,000 square feet of new lab and office space, citing growing demand from early-stage biotechs. The expansion is expected to create space for up to 10 additional companies. Also in North Chicago, home-grown AbbVie announced plans to build two new API manufacturing facilities totaling $380 million at its campus in the Chicago suburb. The facilities—designed to support production of next-generation neuroscience and obesity treatments—are set to be fully operational in 2029. However, AbbVie opted to build its planned $1.4-billion biomanufacturing campus not in North Chicago but 821 miles southeast in Durham, NC. Across Illinois, biotech stakeholders have applauded Gov. J.B. Pritzker (D) for proposing to sweeten the state’s Research & Development Tax Credit program by allowing companies to transfer their credits for cash. “This is a transformative step for our startup and growth-stage ecosystem,” stated John Conrad, president and CEO of the Illinois Biotechnology Innovation Organization (iBIO). Pritzker is seeking a third term in November vs. Darren Bailey (R).
The Windy City and vicinity rank sixth in both NIH funding (2,658 awards totaling $1.607 billion) and jobs (94,000, according to statewide industry group Illinois Biotechnology Innovation Organization or iBIO). The region places ninth in patents (5,569 families) and VC ($917.677 million in 2025, says iBIO, zero in Q1 2026,
10. Seattle
AGC Biologics, a global CDMO, expanded its regional research footprint last fall by signing a 37,575-square-foot lease at Element Research Center in Bothell, WA. [AGC Biologics]
Seattle and the Greater Puget Sound’s strong base of academic and other nonprofit research institutions helped the region achieve consecutive years of Nobel laureates: Mary E. Brunkow, PhD, of the Institute for Systems Biology in Seattle co-won the 2025 prize in Physiology or Medicine a year after David Baker, PhD, director of the Institute for Protein Design at University of Washington (UW), co-won the 2024 prize in Chemistry. A UW spinout, Seattle-based 3D tissue model developer Curi Bio, closed in December on a $10-million Series B financing led by South Korean contract research organization DreamCIS. In April, Achieve Life Sciences (based in Seattle and Vancouver, BC) announced an up-to-$354 million private placement whose purposes include funding a Phase III trial and future commercialization of e-cigarette cessation candidate cytisinicline, while Athira Pharma landed up to $236 million in conjunction with acquiring exclusive rights from Sermonix Pharmaceuticals to the Phase III metastatic breast cancer candidate lasofoxifene. AGC Biologics, a global CDMO, expanded its regional research footprint last fall by signing a 37,575-square-foot lease at Element Research Center in Bothell, WA. However, Astellas Pharma told Washington state officials in April it will shutter the Seattle site of its Universal Cells subsidiary by 2028, with 50 employees to be impacted via layoffs or transfers to South San Francisco, CA, or Westborough, MA.
Seattle and its suburbs placed highest at eighth in both NIH funding (eighth with 1,892 awards totaling $1.572 billion) and VC ($1.06 billion in 2025, zero in Q1 2026, according to industry group Life Science Washington). The region was ninth in lab space (11.46 million square feet, according to regional real estate firm Flinn Ferguson Cresa) and 10th in both jobs (48,765 according to Life Science Washington) and patents (5,416 families).
In April 2025, the U.S. Food and Drug Administration (FDA) released a strategic roadmap to make animal testing the exception for preclinical safety and toxicity studies within the next three to five years. Central to that vision is the adoption of validated new approach methodologies (NAMs), including organ-on-chip systems. The National Institutes of Health reinforced that shift the same month by requiring that all new notices of funding involving animal models incorporate human-focused approaches such as organ chips and other NAMs. Similar changes are emerging globally. In November 2025, the U.K. government published its roadmap to largely phase out animal testing in research while accelerating the development and validation of alternative methods.
For organ-on-chip developers, growing interest from federal agencies is a welcome trend. They are currently generating the data necessary to show that their technologies can work in stringent regulatory environments. However, there are still outstanding questions around validation standards, regulatory expectations, and how NAM data will be evaluated in submissions. At the same time, adoption remains slow, with drug developers continuing to rely largely on established animal models, which command billions in investment compared to the much smaller organ-chip sector.
Still, it is clear that momentum is building behind NAMs. And in response, organ-chip developers are stepping up to ensure that their platforms can produce results when the time comes.
From space flight to lab scale-up
When the Artemis II astronauts launched their historic 10-day journey around the Moon in April 2026, they carried some unusual cargo: organ chips containing cells from their bone marrow. The chips are part of the AVATAR (A Virtual Astronaut Tissue Analog Response) investigation, which is using organ-on-chip devices to study the effects of deep-space radiation and microgravity on human health.
Emulate’s organ chips played a pivotal role in the recent Artemis II lunar mission. The so-called AVATAR experiment could change how space agencies study the effects of radiation and microgravity impact human health. [Emulate
Before the trip, cells from the astronauts were harvested to create two sets of bone marrow chips: one set traveled beside the crew aboard their spacecraft, while another remained on Earth. The idea was to compare both sets of chips when the astronauts returned to Earth. More broadly, the AVATAR project also aims to provide proof-of-concept for including human organ chips in future missions.
In 2025, Emulate announced that its organ-chip technology was selected to accompany the astronauts on their lunar fly-by. It is an exciting project for Emulate, which commercializes human organ-chip technology developed at the Wyss Institute for Biologically Inspired Engineering at Harvard University. But it is only one of several activities that the company has been involved in the recent past. The company’s liver organ chips were one of the first to be accepted for the FDA’s Innovative Science and Technology Approaches for New Drugs (ISTAND) program, which supports tools that fall outside the scope of existing qualification programs but may still be useful for drug development.
Lorna Ewart, PhD Chief Scientific Officer Emulate
In a conversation with GEN, Lorna Ewart, PhD, Emulate’s chief scientific officer, described 2025 as a pivotal year both externally—with announcements from multiple federal agencies promising increased support for organ chips—and internally, with the launch of Emulate’s new instrument, AVA, in June 2025 to address what Ewart describes as “key operational challenges” with the company’s first-generation platform. AVA has a higher throughput than its predecessor, enabling microfluidic workflows across 96 parallel organ chips or “emulations” in a single run. The company claims that it is the first organ-on-chip workstation to combine high-throughput microfluidic tissue culture with automated imaging in a self-contained environment.
Interest in the instrument to date has come primarily from large pharmaceutical companies and mid-sized biotech firms, who need to run large numbers of chips in parallel. But, Ewart says, there is also strong interest from academic institutions and government agencies. Some of that interest is driven by AVA’s much smaller footprint. Compared to Emulate’s first-generation system, AVA is a compact benchtop system that does not require multiple incubators. The company has also reduced the size of each emulation, or chip equivalent, by about 50%, meaning that the new platform requires fewer cells and uses less media, helping to keep experimental costs down. “Academics are actually quite excited about getting their hands on it and looking at it as a core lab instrument where multiple labs will be able to use it.”
AVA also addresses concerns about reproducibility, a consistent source of worry for drug developers, and one that Emulate has made a priority. The company has shared data showing that its liver-chip biology is reproducible both internally and externally in laboratories using AVA. The company has also taken steps to minimize technical variability within experiments as well as bias when running AVA at scale. “We need to make sure that the first chip array looks the same as chip array eight,” Ewart says. “If it doesn’t, there’s variability across those different [chip arrays] that will impact the way that a user can design, what we would refer to as a fully burdened experiment.”
More complex, automated models
When it first launched, U.K.-based organ-on-chip company CN Bio started with a liver-on-a-chip platform, but has since expanded to include various organ models, including intestine, lung, and kidney. The company’s commercial platform is built on technology developed in the laboratory of Linda Griffith, PhD, at the Massachusetts Institute of Technology.
Tomasz Kostrzewski, PhD Chief Scientific Officer CN Bio
Currently, CN Bio has applications in multiple arenas, including safety, toxicology, and disease modeling. “For example, in the toxicology space, we have a very well-known and well-utilized model of drug-induced liver injury,” Tomasz Kostrzewski, PhD, the company’s CSO, tells GEN. That model is being utilized by several global clinical research organizations to offer assays as a service. The company also has a multi-organ system that links its intestine and liver chip models, which can be used to predict the oral bioavailability of drugs, and a range of disease models for metabolic liver disease, chronic obstructive pulmonary disease, and more.
Perhaps one of the biggest challenges, from Kostrzewski’s perspective, is the misconception among some stakeholders that organ chips can fully replace animal models today. That is not a position that the organ-chip community has advocated for, he says. The focus should be on “using these tools to answer the right question and [in] the right context of use at the right time alongside all those other approaches that are out there.”
Development plans in the near future involve making incremental improvements that refine CN Bio’s platform over time. “One key area that we’re working on is immunology and adding in more complex immune cultures into our chips,” Kostrzewski says. Recently, “we presented some of the first data [incorporating] peripheral immune cells in our liver model and looking at the toxicity of monoclonal antibodies.” Some customers are building “neuronal blood brain barrier models on our platform” with an eye towards “understanding how drugs can penetrate across that barrier.” In parallel, the company is expanding into new organ systems, including kidney models, via partnerships.
The company is also turning to automation to help customers scale their work. CN Bio’s open design integrates well with standard robotic systems, making it well-suited for high-throughput workflows, Kostrzewski says. Customers could run more chips in parallel as part of larger screening studies with more consistency and less human intervention. There is also the potential to incorporate sensing capabilities, much like those used in biomanufacturing, to monitor system performance in real time and generate functional readouts.
In addition, the company is working to demonstrate to drug developers that organ chips can generate valuable translational data that predicts clinical outcomes. That certainly has been true for CN Bio as “we have a number of molecules that we have helped take to the clinic” that have been proven successful, says Kostrzewski. And there are customers using its organ chips “to make no-go decisions” regarding potential drug programs. “That’s the ultimate proof that these technologies do what they say,” he says.
CN Bio’s PhysioMimix supports studies of metabolic liver disease, chronic obstructive pulmonary disease, and drug delivery in the brain. There are also efforts to develop additional organ systems using the technology. [CN Bio]
Digital twin and multi-organ models
Hesperos’ co-founders, James Hickman, PhD, and Michel Shuler, PhD, have been involved in the organ-chip space since its early conception. In fact, the technology that underpins the company’s services emerged from work that both scientists were doing independently in their laboratories. Today, the company provides drug development services using its Human-on-a-Chip® single- and multi-organ systems in areas such as neurodegenerative disease.
In April, the company published a study in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association focused on familial Alzheimer’s disease (fAD). Specifically, scientists at Hesperos and the University of Central Florida (UCF) used a neuromuscular junction (NMJ) multi-organ chip to show that fAD-associated mutations caused specific impairments in NMJ functions that occurred independently of brain pathology. Building on that work, Hesperos scientists and their collaborators are trying to understand what therapeutics could potentially be useful for both the peripheral and central nervous systems, as well as which would need to be specific for each.
Last year, the company also demonstrated what they claim is the first true digital twin capability using an organ-on-chip platform. That capability is described in an Advanced Science paper where the scientists explain how a multi-organ system comprising human liver, spleen, endothelial tissues, and blood was used to replicate the full lifecycle of Plasmodium falciparum, the parasite responsible for malaria. They plan to publish additional studies on their work on digital twins. Additionally, like Emulate, Hesperos is also participating in the FDA’s ISTAND program.
James Hickman, PhD Co-founder Hesperos
In a conversation with GEN, Hickman described the broader adoption of organ-on-chip technology as a mixed bag, with some people being more open to the technology and others showing more resistance. He noted that many in the community are still accustomed to using animal models, which may make them more reticent to change, but also acknowledged that animal testing is a multi-billion-dollar business. “There are a lot of people with a vested interest in keeping animal experimentation going,” he says. That means that although people may be interested in alternatives like organs-on-chips, from a practical perspective, it may be difficult for them to disengage from their reliance on animal models.
He also pointed to the FDA’s evolving guidance on alternative technologies—and the lack of clarity—as one of the biggest hurdles. “People are still trying to get their hands around the FDA announcements on moving away from animal models,” and trying to understand what the agency wants to see, Hickman explained. “We have a pretty good idea of what that [might be needed and] we work with a couple of people [to] generate data along those lines,” he says. “The biggest thing is to start getting [clearer guidance] in terms of what they will accept in lieu of safety data.” There are also questions around whether good laboratory practice (GLP) requirements for these new approach methodologies need to mirror those for animal studies, given the differences between the systems. “Doing GLP is really expensive,” Hickman said, and requiring the same standards could effectively put many companies out of the running to conduct safety studies because they can’t afford it.
Equally important is addressing the limited investment in organ chip and other alternative technologies. Hickman estimates that commercial NAM entities collectively generate hundreds of millions in revenue, compared to tens of billions secured by large animal CROs. Although federal agencies have committed to supporting NAMs, providing millions in funding, greater investment is needed for these alternative technologies to come into their own. Hickman added, “It’s a matter of trying to increase that capacity to really start showing that it’s a force in the industry versus a shiny new toy that people haven’t quite figured out what to do with.”
BackgroundDepressive symptoms are common among patients with cancer and can substantially impair quality of life, treatment adherence and overall well-being. Although exercise has been increasingly recognised as a promising non-pharmacological strategy for alleviating depression in oncology settings, existing evidence has focused predominantly on breast cancer, with limited attention to lung and digestive cancers. This meta-analysis aimed to evaluate the effects of exercise interventions on depressive symptoms in adults with lung and digestive cancer.MethodsA systematic search was conducted in PubMed, Web of Science, Embase, Cochrane Library and Scopus from database inception to March 2026. Randomized controlled trials investigating the effects of exercise interventions on depressive symptoms in adults with lung or digestive cancer were included. The primary outcome was depressive symptoms measured using validated instruments. Subgroup analyses were performed according to intervention format, exercise type and training frequency. Risk of bias was assessed using the Cochrane Risk of Bias tool version 1.ResultsEight randomized controlled trials were included in the meta-analysis. Baseline analysis showed no significant difference in depressive symptoms between the exercise and control groups before intervention. Post-intervention meta-analysis demonstrated that exercise significantly reduced depressive symptoms compared with control conditions (SMD = -0.45, P = 0.02), Although substantial heterogeneity was observed. Individually delivered programmes, walking-based exercise and moderate-frequency training (3–5 times per week) showed numerically larger effect estimates.ConclusionsExercise interventions may reduce depressive symptoms in adults with lung and digestive cancer and represent a promising adjunctive strategy for psychological care in these populations. Although subgroup differences were not statistically significant, certain intervention characteristics may be associated with greater benefit. Further large-scale, high-quality randomized trials are needed to confirm these findings and to establish the optimal exercise prescription for reducing depressive symptoms in adults with lung and digestive cancer.Systematic review registrationhttps://www.crd.york.ac.uk/prospero/, identifier CRD420261336578.
ObjectiveThe comorbidity of pain and depression is prevalent, adding difficulty to the treatment of depression. This systematic review with meta-analysis aims to determine the efficacy and safety of acupuncture in treating depression-associated chronic pain (DACP).MethodsA comprehensive search was conducted across four international databases, namely PubMed, Embase, Web of Science, and the Cochrane Library, along with four regional databases, including Wanfang Data, CNKI, VIP database, and SinoMed, from inception to March 2025. The Cochrane Risk of Bias 2 tool was utilized to assess risk of bias in the included research articles, and the Grading of Recommendations Assessment, Development, and Evaluations system was employed to evaluate the certainty of evidence. Meta-regression analysis was performed to explore the influence of patient age and treatment duration on the study results, and sensitivity analysis was used to verify the stability of the results. The publication bias was evaluated when the number of included studies exceeded ten. All data analyses were completed using Stata15.1.ResultsTen randomized controlled trials involving 761 participants were included. Acupuncture combined with conventional medications was more effective than medication alone in improving depressive symptoms (standardized mean difference (SMD): -0.72; 95% confidence interval (CI): -0.91 to -0.53; P < 0.01) and reducing pain (SMD: -0.85; 95% CI: -1.36 to -0.34; P < 0.01). Head-to-head comparisons revealed that acupuncture is similar to medication in improving the Hamilton Depression Rating Scale scores (SMD: -0.05; 95% CI: -0.61 to 0.51; P > 0.05) and the Visual Analogue Scale scores (SMD: -0.33; 95% CI: -0.94 to 0.29; P > 0.05), suggesting no statistically significant difference between the two treatments. In contrast, acupuncture was associated with a better safety profile (relative risk: 0.40; 95% CI: 0.27 to 0.60). Further subgroup analysis found the advantage of a 4-week acupuncture treatment in improving depressive symptoms, while longer-term treatment tended to be more effective in relieving pain.ConclusionsAcupuncture appears to have comparable antidepressant and analgesic effects to conventional oral medications. When applied as an adjuvant therapy, acupuncture may enhance the clinical efficacy of monotherapy for DACP. Regarding treatment duration, a 4-week acupuncture intervention may be superior to a longer cycle (> 4 weeks) in alleviating depressive symptoms, while long-term acupuncture treatment may provide greater benefits in analgesia.Systematic Review Registrationhttps://www.crd.york.ac.uk/PROSPERO, identifier CRD420251026454.
Historical data indicate that animal models are not ideal for the determination of the efficacy and safety of human therapeutics. Ninety percent of drugs that pass animal studies do not receive regulatory approval. Improving predictive accuracy in preclinical tests is paramount, thus the movement toward more human-relevant models.
The goal to reduce the use of animals in preclinical testing changes testing paradigms. In April 2025, the U.S. FDA’s Roadmap to Reducing Animal Testing in Preclinical Safety Studies outlined a strategic, stepwise approach to replace animal testing with scientifically validated new approach methodologies (NAMs), such as organ-on-a-chip systems, computational modeling, and advanced in vitro assays. FDA Modernization Acts 2.0 and 3.0 facilitated this activity by empowering the agency to accept NAMs in lieu of animal studies.
Meanwhile, legislation from the EU, Directive 2010/63/EU, requires marketing authorization holders to integrate the 3Rs (Reduction, Refinement, and Replacement) and welfare standards for the treatment of animals in all aspects of the development, manufacture, and testing of medicines. In addition, last year, the U.K. delivered an expedited phase-out plan for animal use.
But it all began in 2020 with the launch of the FDA Innovative Science and Technology Approaches for New Drugs (ISTAND) pilot program to provide a pathway to qualify novel drug development tools (DDTs) that did not fit within the agency’s existing qualification programs. Qualified DDTs are defined as having a proven, specific use and can be incorporated in any drug development program for a particular context of use.
The pilot has advanced to a permanent DDT qualification program. To date, ISTAND has accepted eight submissions–two tools that assess preclinical safety without using animals, two methods involving tissues, and one statistical approach.
The rigorous ISTAND process
In a 2022 Communications Medicine study to test drug-induced liver injury (DILI), 870 human Emulate Liver-Chips created with cells from three different human donors were challenged with 27 different drugs. The human Liver-Chip predicted human DILI with 87% sensitivity and 100% specificity, ~7 to 8 times more accurate than the comparable animal models.1 These results prompted Emulate to submit a Letter of Intent (LOI) to ISTAND in 2024.
ISTAND accepted Emulate’s LOI for the first organ-on-a-chip DDT to predict DILI. The human Liver-Chip S1 was proposed to assess the risk of small molecule candidate drugs inducing DILI in adults to create human-relevant data for candidate drug IND submission.
The LOI acceptance was the entry point in a three-step rigorous qualification process. ISTAND required Emulate to qualify the in vivo-like physiological functionality of the Liver-Chip S1, and quantify its ability to predict DILI risk through changes in tissue morphology as well as alterations in albumin and alanine transaminase (ALT) protein concentrations when the chips were challenged with toxic drugs administered across eight concentrations.
Now, the Emulate Liver-Chip S1 is in the final stages of qualification. Two independent commercial users need to successfully produce similar results. Pending successful completion, the Liver-Chip will be the first FDA-approved DDT to assess the potential of a small-molecule candidate drug to cause DILI when a prior structurally similar small-molecule has shown DILI in the clinic.
High-throughput capabilities
Moving toward reduction and, in some cases, replacement of animal models demands both biological fidelity and throughput. For model development and target validation, the Zoë-CM2® Culture Module automates the precise condition needed to culture up to 12 chips.
For high-throughput options, the AVA Emulation System is a self-contained Organ-on-a-Chip workstation that fuses high-throughput microfluidic tissue culture, full environmental control, and real-time imaging into a single, compact benchtop unit. The Chip-Array
consumable integrates 12 independent Organ-Chips into an SBS format for 96-well streamlined workflows with multichannel pipettes and automated liquid handlers.
Reference
1. Ewart, L., Apostolou, A., Briggs, S.A. et al. Performance assessment and economic analysis of a human Liver-Chip for predictive toxicology. Commun Med 2, 154 (2022). doi.org/10.1038/s43856-022-00209-1.
















 Emulation System is a self-contained Organ-on-a-Chip workstation that fuses high-throughput microfluidic tissue culture, full environmental control, and real-time imaging into a single, compact benchtop unit. The Chip-Array
Emulation System is a self-contained Organ-on-a-Chip workstation that fuses high-throughput microfluidic tissue culture, full environmental control, and real-time imaging into a single, compact benchtop unit. The Chip-Array