WASHINGTON — Health secretary Robert F. Kennedy Jr. on Wednesday pointed to his “publicly available calendar” as an example of his commitment to transparency and to beat back unfavorable reporting.
But no such calendar, detailing who Kennedy meets with or how he spends his time, has been released by the administration. STAT has been asking the Department of Health and Human Services for Kennedy’s calendar for more than a year, via Freedom of Information Act requests and emails to the press office.
New data released Thursday suggest the prevalence of drinking during pregnancy increased in recent years.
National survey data published in a Centers for Disease Control and Prevention report show about 15% of adult pregnant women reported current drinking (use in the prior 30 days) between 2021 and 2024. About 13.5% of women reported the same between 2018 and 2020.
You’re reading the web edition of STAT’s Health Tech newsletter, our guide to how technology is transforming the life sciences. Sign up to get it delivered in your inbox every Tuesday and Thursday.
Good morning health tech readers!
I’ve been a remote worker since early March 2020. Even if it suits me fine, I was surprised to learn it might be ruining my life.
Sara Barrington is CEO of Verici Dx, a precision diagnostics company redefining how transplant clinicians understand and predict graft health. By combining multi-omic analysis with proprietary artificial intelligence (AI) models, Verici Dx delivers predictive, actionable intelligence that helps clinicians optimize therapy, inform biopsy decisions, and stratify risk for complex transplant patients.
In this edition of Asked & Answered, Barrington speaks with Inside Precision Medicine Editor in Chief Damian Doherty about pioneering innovation in transplant diagnostics to better reflect biological and patient complexity, and ultimately, improve health outcomes.
Q: Tell me about Verici Dx, its founding, mission, and products.
Sara Barrington: Verici Dx was founded with a very clear purpose: to fundamentally improve how transplant clinicians are informed and manage graft health. Transplant medicine requires high-stakes, time-sensitive decision-making to promote longevity of the graft, minimize the risk of complications, and improve the patient’s quality of life.
Sara Barrington
Kidney transplantation has long struggled with one fundamental challenge: accurately identifying rejection early and distinguishing it from other causes of injury and graft dysfunction. Clinicians often rely on conventional blood markers such as serum creatinine or, more recently, donor-derived cell-free DNA. While these tools are useful for signaling that “something is wrong,” they are injury markers and lack a level of precision important in rejection biology.
Creatinine levels, for example, increase only after functional damage has already occurred and cannot differentiate rejection from non-immune causes of injury such as ischemic reperfusion injury, drug toxicity, or viral infections like BK virus–associated nephropathy. Biomarkers can generate false positives, triggering biopsies or treatment escalation that may not be necessary and can expose patients to avoidable risk.
This lack of specificity has made rejection difficult to manage proactively. By the time rejection is clearly identified, tissue injury may already be established. At the same time, clinicians are understandably cautious about intensifying immunosuppression without clear evidence, given the associated risks of infection, malignancy, and toxicity.
Our mission is to close this information gap by delivering precision diagnostics that reflect the true complexity of transplant biology and translate that complexity into insights clinicians can proactively and confidently apply to patient care.
We operate at the intersection of multi-omic science, advanced analytics, and clinical reality. We know that transplant rejection and graft injury are not single-signal events, but are multifactorial, dynamic biological processes. We design our diagnostics to capture that complex biology in a way that mirrors how clinicians think about their patients, rather than forcing clinical decision-making to fit the limitations of older technologies.
Our lead product, Tutivia, is a blood-based test that assesses the immune and broader, relevant biological status of kidney transplant patients to identify the risk of all forms of acute rejection, including T cell (TCMR) and antibody-mediated rejection (ABMR). Tutivia combines transcriptomics with proprietary AI models to address this precise unmet need: biologically accurate insight into what is actually happening within the graft.
The test delivers a risk score that enables more precise immunosuppression management by distinguishing rejection from other causes of graft injury, such as BK virus–associated nephropathy and ischemia-reperfusion injury, which can confound conventional blood tests like serum creatinine and donor-derived cell-free DNA.
By focusing on the immune and other pathways associated with rejection, Tutivia moves beyond damage markers and toward a direct assessment of rejection biology itself. That shift, from injury detection to biological interpretation, is what makes the test such a valuable tool for transplant clinicians.
Thermo Fisher Scientific recently launched its One Lambda Pre-Transplant Risk Assessment (PTRA) assay, using pre-transplant prognostic technology licensed from Verici Dx. The assay provides a risk score for early acute rejection based on a patient’s unique gene profile, helping clinicians better balance the risk of rejection against the potential side effects of over-immunosuppression. Using a 29-gene mRNA signature, the PTRA assay stratifies patients into high- and low-risk categories, with clinical validation showing high-risk patients are seven times more likely to experience early acute rejection.
Q: Tutivia is built on RNA sequencing. Why is precision transcriptomic analysis well-suited for identifying rejection biology?
Barrington: The need for reliable biomarkers is crucial for individualizing therapy that offers the potential to extend allograft survival.
Early research underpinning the science leading to the development of Tutivia was led by principal investigators at The Mount Sinai Hospital in New York, one of the world’s leading transplant research centers, combining decades of clinical expertise with rigorous science. The underlying science reflects the fact that rejection in kidney transplant patients is not driven by a single molecule or pathway, it results from coordinated immune and other biologic pathways across multiple cell types, signaling cascades, and regulatory mechanisms. Injury-driven biomarkers capture only a narrow slice of this biology and can be influenced by non-rejection factors, limiting their specificity and reliability.
Precision transcriptomic analysis, on the other hand, measures gene expression patterns across thousands of genes simultaneously. In developing specific tests, this analysis is the basis for gene selection using unsupervised deep learning mathematical modeling, allowing the most impactful and reproducible gene expression signals and interactions to be included in the final signature.
Tutivia uses a peripheral blood next-generation sequencing assay to evaluate a 17-gene mRNA signature in combination with a proprietary artificial intelligence algorithm to categorize kidney transplant patients as at low risk or high risk of acute rejection.
This provides a comprehensive view of immune activation, regulation, and injury responses within the transplanted organ, allowing the identification of signature changes that are truly characteristic of rejection biology.
In short, RNA sequencing lets us ask better biological questions: not just whether the kidney is injured, but whether immune-mediated rejection is driving that injury. That distinction is critical for precision medicine in transplantation.
Q: What does earlier and more precise identification of rejection biology mean for patient management and outcomes?
Barrington: Earlier identification of rejection biology can create an opportunity to intervene before irreversible damage occurs. When clinicians have confidence in what the biology is telling them, they can make timely, targeted decisions that may preserve graft function.
This precision also supports more individualized care. Rather than applying broad treatment strategies, clinicians can tailor immunosuppression based on biological risk, potentially reducing over-treatment and its associated complications.
For patients, this can translate into fewer unnecessary biopsies, fewer adverse events related to immunosuppression, and a greater likelihood of long-term graft survival. Ultimately, better information leads to better decisions, and better decisions lead to better outcomes.
Our vision is that precision diagnostics like Tutivia become a standard component of transplant management, providing earlier insight into rejection biology, supporting more informed clinical decisions, and helping clinicians intervene at the right time for the right patient.
Q: AI is central to your platform. How does Verici Dx apply AI differently from others in diagnostics?
Barrington: We apply AI with rigor and restraint. We use advanced machine learning and mathematical modeling to analyze highly complex biological data, but always within a disciplined scientific framework. Our models are developed using unsupervised approaches and validated extensively on inclusive patient populations. Once validated, they are locked and reproducible; they are not evolving over time. That distinction matters because clinicians are making life-altering decisions based on these results, and trust, consistency, and validation are essential.
Q: Validation and standards are recurring themes for Verici Dx. How was Tutivia validated?
Barrington: Tutivia was validated through a rigorous clinical study that included a broad and diverse transplant patient population, rather than narrowly curated cohorts. We deliberately chose a more difficult validation path because clinical reality is complex, and diagnostics must perform under those conditions. While this approach requires more time and effort, it ensures the test is reliable, reproducible, and clinically relevant across the full spectrum of patients that clinicians see every day.
Q: What’s in the future for the company?
Barrington: Verici Dx is focused on deepening the clinical adoption of Tutivia as well as expanding the studies demonstrating the utility of an earlier and more precise biomarker in improving patient outcomes. Long-term outcomes for transplant patients involve more biological pathways, and significant complexity is involved in managing care. We are focused on developing and validating tests using both transcriptomic and proteomic precision tools to assist clinicians and their patients in this journey.
Damian Doherty has been in media and publishing for over 30 years, beginning at News Corporation. Damian has managed, edited, and launched life science titles in drug discovery and precision medicine. He was features editor of Drug Discovery World and founded the Precision Medicine Leaders Summit and the Journal of Precision Medicine. He edited AIMed magazine before launching Photo51Media, a platform for illuminating untold, compelling stories in precision healthcare. Damian joined Mary Ann Liebert in 2021 to help steer the new rebrand and relaunch of Clinical OMICS to Inside Precision Medicine.
Background: Physical activity (PA) is a promising prevention approach for supporting mental health and enhancing social inclusion among postsecondary students. However, it is unclear whether similar outcomes are realized when PA programming is delivered in-person versus virtually. Objective: Using data from a multiphase research project, the purpose of the study was to examine the influence of on-campus PA programming (virtual and in-person delivery) on mental ill health symptoms (ie, anxiety and depression), social inclusion indices (ie, social connectedness, emotional ties, and social relationship quality), and well-being. Three objectives were addressed: (1) to assess pre-post change in symptoms, social inclusion indices, and well-being for virtual and in-person delivery; (2) to evaluate whether outcome change over time differed by delivery mode; and (3) to examine whether change in symptoms and social inclusion indices predicted change in well-being for both delivery modes. Methods: Physically inactive postsecondary students experiencing mental ill health participated in a 6-week structured and supervised PA program. Pre-post intervention data were collected across 3 phases, and the analytical samples included: 1. In-person delivery (n=87; 82%, 69/84 young adults; 86%, 74/86 women; 38%, 33/86 White; 20%, 17/86 Chinese; 86%, 75/87 with mental illness; 2. Virtual delivery (n=62; 69%, 42/61 young adults; 95%, 59/62 women; 34%, 21/62 White; 21%, 13/62 South Asian; 55%, 34/62 with mental illness), and 3. Data from students who received in-person or virtual delivery: (n=92; 67%, 61/91 young adults; 90%, 83/92 women; 32%, 29/92 White; 20%, 18/92 South Asian; 59%, 54/92 with mental illness). Data were analyzed using 2-tailed paired samples tests to address objective 1, a 2 (delivery mode) × 2 (time: pre-post) repeated-measures ANOVA to address objective 2, and hierarchical regression analyses to address objective 3. Results: Both virtual and in-person PA delivery were effective for symptom reduction and social inclusion improvements across all outcomes (<.001), with moderate-to-large effects. There was no significant time × delivery mode (=0.72, ²=0.04, =.60) interaction effect. Change in social inclusion indices explained unique variance in well-being, beyond covariates (gender, mental illness, and ethno-racial identity), and symptom reduction for virtual ( = 0.75, 008001) and in-person ( = 0.72, =0.16, <.001) PA delivery. Conclusions: Online distance learning is increasing across postsecondary settings worldwide, underscoring the need for accessible, technology-enabled mental health prevention interventions. The results provide support for the effectiveness of virtual and in-person PA programming for reducing symptoms of anxiety and depression, while also enhancing social inclusion indices and overall well-being. Social inclusion indices were also a key contributor to improved well-being, emphasizing the relevance of social factors in both virtual and in-person PA-based mental health prevention strategies for postsecondary students.
Despite an estimated 190 million women and girls around the world living with endometriosis, a chronic and painful gynecological condition, no disease-modifying therapy has yet been approved to treat it. Léa Wenger, PhD, and her colleagues at Cyclana Bio are aiming to fix this.
Endometriosis occurs when endometrial tissue grows outside the uterus, causing inflammation, pain, and sometimes scarring and fertility problems. Although this condition was historically neglected in terms of research and development, Cyclana is now one of a small but growing group of companies trying to develop more effective endometriosis treatments. After completing a veterinary degree, Wenger shifted away from clinical practice when she discovered a passion for biomedical research during her PhD at the University of Cambridge. During this time, Wenger was diagnosed with endometriosis, which led her to co-found Cyclana Bio in 2024 with Kevin Chalut, PhD, who was her colleague at Altos Labs at the time.
The company joined the Babraham accelerator program last year and has already raised an oversubscribed £5 million ($6.8 million) pre-seed round. Wenger spoke to Inside Precision Medicine’s senior editor, Helen Albert, about her inspirations, career, and what she and her colleagues are hoping to achieve at Cyclana.
Q: What inspired you to become a scientist?
Léa Wenger, PhD
Léa Wenger: I was always very curious as a child. What drove me directly to science, rather than going for any other subjects, was my desire to be a vet. I wanted to be a vet and knew vets needed to know about science, so I decided to learn all the science I could. The irony of that was that I didn’t end up practicing a single day of veterinary medicine, but it got me into the doors of institutions where they teach you veterinary medicine in a way that was very scientific and research-driven. I really discovered a passion for science at that point, a passion for actually understanding things that we don’t know. I was exposed to this idea of driving knowledge where it isn’t present, and that was really what got me excited about research. That’s when I effectively shifted from the veterinary medicine career to the more traditional biomedical research route.
Q: What made you decide to go into biotech rather than staying in academia?
Wenger: I think the frustration I had in academia was that the system was set up to do a one-person, one-project type of research. That can be fun in some ways, but for me, it didn’t really address impact in the way that I really wanted it to. I wanted to feel like I was working towards creating discovery, translating it, and being able to improve patient lives. I just felt that biotech was a better conduit for that because it was based on faster-moving collaborative teamwork.
I was working in neurodegeneration at the time and on organoid models made of 3D stem cell-derived complex architectures. Organoid models are incredibly good at reproducing human development. But when you’re looking at neurodegenerative diseases that happen with age, it’s a lot harder. Aging in a dish is really hard to reproduce.
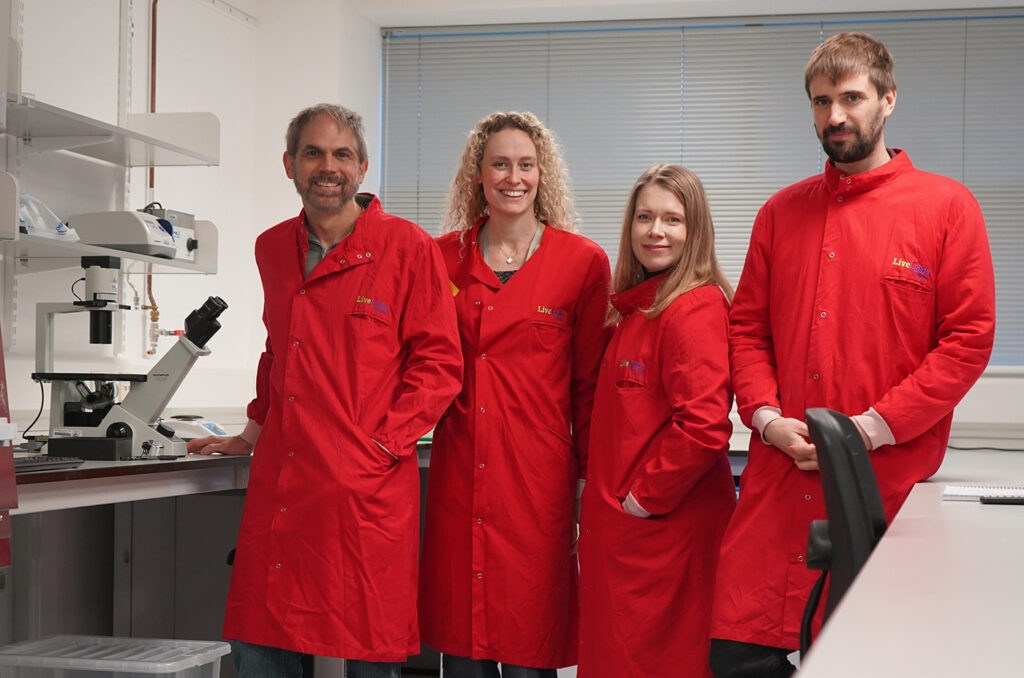
Cyclana Bio scientists working in the LiveLabs laboratory, from left to right, Kevin Chalut, PhD, cso and co-founder, Léa Wenger, PhD, ceo and co-founder, Siiri Salooma, PhD, founding scientist, and Tom Wyatt, PhD, founding scientist.
It was at exactly then that I wanted to go down this research route in more detail that Altos Labs opened in Cambridge. The company had a thesis of “Let’s try and do real discovery science, deep, groundbreaking science,” but in a biotech environment where you’re much more collaborative. That really attracted me at the time, and so I applied to work there after my PhD. Luckily enough, they took a chance on me and believed in me.
I loved it and I learned a huge amount. Not just in terms of how you build discovery programs from the ground up, but also how you work in a team, how you focus, and how you align incentives in biotech. I think it completely shifted my mindset away from simple academic curiosity to, “How do we drive that curiosity towards impact as quickly as possible?” The bar, in my opinion, is somewhat higher than in academia because you’re not just saying, “Is this good enough to publish?” You’re saying, “Is this a therapy? Is this actually good enough to put into a human and help them and not harm them?”
Q: What made you decide to found Cyclana Bio?
Wenger: I was in an epigenetics lab within Altos, and my co-founder was actually one of the group leaders there working on the extracellular matrix. The more I worked with him, the more I realized how massively important it is in guiding how cells behave. You can get completely different responses from a cell depending on what environment it’s in. I got really interested in that interface between the epigenetics, the gene level regulation, and the [extracellular] matrix.
I was doing a lot of discovery science there, but during that time, I also developed endometriosis. I was in my mid-to-late 20s when my symptoms started, and they got worse very quickly. Like every scientist who gets diagnosed with a condition, I nerded out on the disease. In my spare time, I downloaded all the data and looked into what research was there, and very quickly realized that there wasn’t much information available.
There’s not much that we know about the disease and how it happens. People are still debating the causes and drivers of endometriosis. That was interesting and another area of unknown, which has always been what I was attracted to. I’d always been passionate about women’s health, but never really had the opportunity to do something about it.
There’s an easy, non-invasive way of getting access to cells to study endometriosis because menstrual fluid is built and shed every month from your endometrium. It’s built and shed in healthy women, in women with endometriosis, and in women with other conditions. On top of that, biopsies are actually way more common in gynecology than in a lot of other conditions. So I realized this was a huge opportunity to do this tissue-level discovery that we were so passionate about, but for a cause that I really believed in, in a field that was unknown.
I spoke to the CEO at Altos at the time and explained what I wanted to do. He was supportive and thought it was an interesting idea, but ultimately, the indication didn’t align with the priorities of Altos—of looking into age-related diseases. So that’s when we left and started Cyclana Bio.
Q: How easy was it to start the company?
Wenger: We were very lucky in that we got into the Babraham accelerator program very quickly, last May. That was important because not only did it give us validation that someone had actually picked us and said this is a good idea, but it also gave us lab space and access.
We did take quite a bit of a risk. Both my co-founder and I left without having raised funding or grants to start the company. For a short while, we were living off our savings and also paying for some very preliminary science and our first scientist to try and get some data going. That was in May [2025], but quite quickly, we got a bit of traction. By July, we had our first investment term sheet because we started fundraising immediately. Then by September, we were oversubscribed. We finalized the closing in October–November for a £5 million pre-seed round.
I think along the way, we basically just had to assume it was going to happen. We were building the company as if we had the money already, although we were always very open with Tom [Wyatt], the scientist who joined us first, about how much funding we had when he joined.
We’re nine people now and have some amazing scientists who have joined the team, including a great CTO who was also at Altos beforehand. We are still growing as we speak. It’s funny how science brings so much more science.
Q: What are you trying to achieve at Cyclana?
Wenger: Our main aim is to get at least one therapy that’s truly disease-reversing to the clinic. Based on a lot of research, we know that the extracellular matrix can guide how cells respond. It can act as a sink for particular signal factors. Sometimes it can sequester or deliver things like growth factors or inflammatory signals, but it also massively changes how the cell is interacting with its neighbors.
It’s a key component of a positive runaway effect that happens in lots of chronic inflammatory diseases and in some cancers. A lot of the time, when trying to develop treatments, we focus on the cells and whether we can stop that inflammation. What we think is, if you don’t address problems with the matrix, you are not going to cure the disease. You’re effectively just going to mitigate the side effects, and this matrix is going to act like a memory of the disease. This means that if you stop the treatment, it comes back because the matrix issue hasn’t been solved.
We think that that’s a big element of what’s going wrong with endometriosis. Lesions are removed surgically and then they come back. We really think the diseased extracellular matrix is very much driving the pro-inflammatory phenotype, and that if we don’t address that, we don’t actually get to the point where we are curing the disease. We want to see if we can effectively reverse the phenotypes and if we can effectively get to a cure by stopping this recurrent feedback loop.
We haven’t settled on an exact target or modality yet. We’re exploring a few different targets, and I think based on exactly what mechanism we want to go after, we will determine what the best modality is. We want to be sure about the science, very sure about the target, and then make that target work.
Q: Where does precision medicine come into your strategy?
Wenger: Our overall strategy is based on how we see endometriosis as a whole, but I think endometriosis hopefully won’t be viewed like that much longer. We hope that there’s going to be much better stratification and classification of the disease, because it manifests very differently in different women.
Although we think the extracellular matrix might be a common mechanism, we’re building a research platform where we will hopefully find out for sure because we’re collecting data. We’ve got an ongoing observational clinical study where we’re collecting biopsy tissue, menstrual fluids, clinical data, and blood from women, either with or without endometriosis.
We’re collecting that data, looking at the tissue, the proteins, and the architecture, but also isolating cells to test in our models. Then, when we start perturbing with particular interventions that we think might reverse the disease’s impact on the matrix or have different effects on the cells, we might start seeing patterns as to which types of women with endometriosis respond well to different treatments.
It’s going pretty well so far, thanks to our clinical collaborators and participants who have donated samples. Menstrual fluid is a very good way of getting samples from seemingly healthy women, because they don’t need to go to the doctor, [they] just send us a sample. We are also collecting tissue biopsies during routine gynecological procedures to minimize invasiveness and inconvenience.
So far, there’s lots of variability, which was what we expected and which is why we want to collect [samples from] a high number of donors. Not because we think that variability is noise, but because variability is signal. It can tell us more about the nuances of the disease in these different manifestations.
Q: What has the experience of being a CEO and biotech founder been like so far?
Wenger: It’s definitely been a steep learning curve. I think that’s also why it’s been so fulfilling, because I do love being in an environment where I’m not complacent, where I’m always learning.
To some extent, because we had so much freedom at Altos to drive our own projects, I had exposure already to the pure project management side of science, so that didn’t seem quite as much of a step up.
Obviously, there’s a huge business, commercial, and legal dimension that I never had thought about before. But I have been trying to learn as much as I can, as quickly as I can, from others. One thing that the biotech field is quite good at is volunteering information. You go to any sort of networking event, or you meet someone from the industry, and they are often very willing to talk to you about what they’re interested in, but also about what you’re doing, and give any advice they might have.
I’ve met many people who have helped me along the way and who have shared their opinions with me. I walked in expecting academia to be way more collaborative than the biotech industry, but actually, I’ve been very pleasantly surprised with my experience.
Q: Can you share any key learning experiences from the last year?
Wenger: If you have scientific training or you can think in a scientific way, going into the field of business or building a company is somewhat similar. There’s lots of information and lots of alternative paths that you can take, just like in scientific discovery, and there is differently weighted evidence as to which paths are the best ones to take. Once you have a certain amount of information, you can then take the best educated guess. That’s how I’ve gone about building the company. For example, when I started, I was told by a friend, “If you’re starting a biotech, you’re going to need to raise venture capital.” They gave me a book called Venture Deals, which is a very good book that explains how funds work. I read that book and felt I was better equipped to talk to people at the fundraisers. I think the first thing I’d say is, when going into any sort of field, try to really understand how and why that field exists and what are the structures that define its environment. Then you can put context into how people work. As a first-time founder, you might think, “I’m going to find investors, and if they believe in me, they’ll invest.” But there’s so much more to running a venture capital fund. Those things are important to know when framing your discussion.
Something I would do differently is not do everything at once. I left my job, started the company, started the science, started building the network, and started fundraising at the same time. There was always this pressure when I was meeting people that I also had to get them to invest. I think looking back on it, if I could start over, I probably would have spent a few more months trying to build my network and understanding the field better before I started having those investment conversations. It still worked out for us, we still raised funds, but it was stressful. Networking events were very high stakes!
Q: How has the endometriosis space changed in recent years?
Wenger: Gedeon Richter purchasing the Celmatix portfolio and backing FimmCyte are very good signs that people are trying again. I think endometriosis has been plagued by failures in clinical trials, and I think now we’re finally seeing some non-hormonal options being tested, which makes me hopeful. Some will fail, some will succeed, and the successes will drive more interest and availability of funding and hopefully, more successes in the future. I’m really looking forward to seeing the results from some of those clinical trials because I think the more solutions we have for women, the better.
Q: Is funding in the overall field of women’s health changing for the better?
Wenger: Absolutely. I think the funding environment is more open to women’s health. I think that’s been helped by the World Economic Forum and McKinsey Health Institute driving the message of value there. There is excitement, I think, and more funding, especially privately.
I’m not sure about public funding. I do think that on the public funding side, we have a trend of saying, “We should fund women’s health, let’s look for quick wins.” I think that’s a bit of a problem with any field that’s been somewhat left behind, once we realize that we need to bring it back. The risk will be funding the wrong things or putting too much of the money into solutions that may not be revolutionary because they don’t have the foundational science to back them up.
It can also be easy to get stuck in the valley of death between seed and late-stage funding. But I do think that there are incredible scientists moving into the field, and there are some great companies starting up. So even if there is this bias towards pre-seed or seed funding, you only need a couple of those companies to have some really promising data, and they will be funded. The bar might be higher than in other fields, but if you produce groundbreaking discoveries, there will be money.
Q: What advice would you give other new founders starting to build their companies?
Wenger: Just follow your gut and your dream. That’s the most important thing. I started Cyclana because I thought this needed to happen and we needed to look into endometriosis. I thought it was a bit hypocritical of me to think we needed to do something and not do it, despite having the training and the skills to try and find a solution. If you really believe something needs to happen in the world, startups are the best way to feel like you are driving that change and contributing to seeing the change that you want to happen. Whether it succeeds or not, you won’t wake up thinking, “What am I doing this for?” You’ll just be thinking, “I really hope that we don’t fail!”
Helen Albert is senior editor at Inside Precision Medicine and a freelance science journalist. Prior to going freelance, she was editor-in-chief at Labiotech, an English-language, digital publication based in Berlin focusing on the European biotech industry. Before moving to Germany, she worked at a range of different science and health-focused publications in London. She was editor of The Biochemist magazine and blog, but also worked as a senior reporter at Springer Nature’s medwireNews for a number of years, as well as freelancing for various international publications. She has written for New Scientist, Chemistry World, Biodesigned, The BMJ, Forbes, Science Business, Cosmos magazine, and GEN. Helen has academic degrees in genetics and anthropology, and also spent some time early in her career working at the Sanger Institute in Cambridge before deciding to move into journalism.
In a rare move, nonprofit organization Blood Cancer United announced Thursday it was buying the remaining supplies of Luvelta, a discontinued investigational cancer drug.
As part of the transaction, Blood Cancer United, previously known as the Leukemia & Lymphoma Society, also will acquire the investigational new drug designation and manage the compassionate-use program for children with a rare form of blood cancer, distributing the medication to patients at no cost while supplies last.
Researchers in Japan have found that older adults with higher levels of vitamin C in their blood have a higher volume of gray matter in their brains and higher connectivity across brain regions involved in memory and attention. Published in PLOS One, their study raises the possibility of using dietary interventions to protect brain health as we age.
“What I found most fascinating about this research is that we were able to detect these subtle but significant associations between a single nutritional factor and large-scale brain networks by utilizing a robust, community-based cohort of over 2,000 older adults,” said Tomohiro Shintaku, MD, PhD, assistant professor of radiology at the Hirosaki University Graduate School of Medicine. “It truly highlights the potential impact of our everyday dietary habits on our brain structures.”
Previous research had linked diets high in vitamin C with lower risk of developing cognitive impairment in older adults. However, this study is the first to look directly at a potential link between vitamin C levels in blood and changes in brain structure and connectivity within a large participant cohort.
Shintaku and colleagues analyzed magnetic resonance imaging (MRI) scans and blood levels of vitamin C in 2,044 Japanese adults over the age of 64. They measured the volume of gray and white brain matter in each individual, as well as the connectivity between brain regions belonging to the default mode network, which are associated with important cognitive functions including autobiographical memory, future thinking, self-reference, and attention. Connectivity within the default mode network is also known to play a significant role in brain health, with lower connectivity being linked to cognitive impairment and Alzheimer’s disease, in addition to a number of psychiatric conditions including depression or schizophrenia.
After adjusting for other factors that affect brain structure and connectivity, such as age, physical activity, and education level, results showed that higher levels of vitamin C were associated with a higher volume of gray matter across several brain regions, and with higher connectivity within the default mode network.
“Our study demonstrates that higher plasma vitamin C levels are associated with better preserved structural connectivity of the default mode network, a key brain network involved in cognitive function,” said Shintaku. “This finding generates the exciting hypothesis that a diet rich in vitamin C might play a supportive role in maintaining brain health and mitigating age-related cognitive decline in older adults.”
More research will be needed to uncover the potential biological mechanisms driving this association and confirm whether there is a causal link between blood levels of vitamin C and changes in brain structure and connectivity. Going forward, the researchers plan to conduct studies looking at repeated measurements of vitamin C levels over time, accounting for additional lifestyle and nutritional factors that may influence these effects, and including cohorts with more diverse ethnicities and socioeconomic status.
Developing truly disease-changing treatments for Alzheimer’s disease and other neurodegenerative conditions has proved challenging, with many failed trials over the last few decades. The approval of Eisai/Biogen’s monoclonal antibody lecanemab in 2023, the first such treatment to have a positive, albeit modest, impact on symptoms of Alzheimer’s disease, was therefore received with enthusiasm by many.
Critics of lecanemab and Eli Lilly’s donanemab, approved a year later for the same indication, argue that the small benefit gained from the drugs does not outweigh the economic costs, possible side effects, and burden of regular intravenous infusions.
Using a vaccine-style approach, where the treatment prompts the body to generate its own antibodies, has the potential to solve these problems. Several companies are developing active immunotherapies to target Alzheimer’s and Parkinson’s disease, as well as other neurological conditions.
Andrea Pfiefer, PhD CEO and Co-founder AC Immune
“What we’re trying to do is link the antigen to a carrier and bring it into a form which mimics the pathology,” explained Andrea Pfeifer, PhD, CEO and co-founder of Swiss company AC Immune, a leading biotech taking the active immunotherapy route to target Alzheimer’s and Parkinson’s disease.
“We inject it into the immune system, and what it recognizes is the misfolded protein. So, because of that, the immune system only makes antibodies against this pathological protein.”
Although none have yet reached the market, the active vaccine-style approach potentially has a number of advantages over passive treatment with monoclonal antibodies. Importantly, fewer rounds of treatment are required. The exact dosing is yet to be determined, but it would certainly be less frequent than the regular infusions of lecanemab or donanemab that are currently prescribed. This would help reduce costs and treatment burdens for patients and their families. There is also likely to be less risk of amyloid-related imaging abnormalities (ARIA) due to the relatively slower onset of antibody generation by the body.
“If you have to take the patient every two to four weeks to get a two-hour infusion in a hospital, and then you have to wait and do imaging, it’s really burdensome,” said Pfeifer.
“After a certain while, they just don’t want to go. … They say, ‘Sorry, we believe your science, we believe everything, but we don’t want this.”
To date, most vaccine trials have enrolled people with at least some degree of Alzheimer’s or Parkinson’s disease, as preventive vaccine trials need to be large and long in duration. Theoretically, developing a preventive vaccine is a feasible approach, as many neurodegenerative diseases typically have a slow onset before noticeable symptoms appear. However, reliable biomarkers that can accurately predict disease onset have been in short supply.
ALZ-101 – Alzinova’s disease-modifying vaccine candidate for Alzheimer’s disease
This is changing, though. Last year, two blood tests that measure phosphorylated tau and amyloid ratios were approved by the U.S. Food and Drug Administration (FDA) for Alzheimer’s diagnosis. The biomarker field is less developed for Parkinson’s and other neurodegenerative diseases, such as amyotrophic lateral sclerosis (ALS), but things are slowly improving.
Promising mid-stage results from front-runners like AC Immune and Alzinova suggest that this pathway has merit, but whether they can succeed in larger registrational trials going forward is unclear.
Tord Labuda, PhD CEO, Alzinova
“It remains to be seen how our immune system reacts. I think that when we look at the titers we see from the vaccine, they’re similar to what we get with passive immunizations. So I think there are a lot of things that point in the right direction,” said Tord Labuda, PhD, CEO of Swedish biotech Alzinova, which has an amyloid beta vaccine in development.
“Personally, I don’t think that the vaccine or passive immunization is the real challenge. The real challenge is to have the right target.”
Taking a more active approach to immunotherapy
While passive immunotherapies like lecanemab and donanemab are groundbreaking in that they are the first disease-modifying treatments for Alzheimer’s to be approved by the FDA and they slow cognitive decline by around 25%–35% over two years, these drugs can cause significant side effects such as ARIA.
This can cause brain swelling and bleeding in some people. Individuals at highest risk for some neurodegenerative conditions, such as carriers of the APOE4 gene variant, are prevented from accessing these therapies at all, as they have a higher-than-average risk of experiencing ARIA-like side effects.
Treating neurodegenerative diseases like Alzheimer’s and Parkinson’s disease when symptoms commence is problematic, as currently, there is no known method of regaining neuronal function once it has been lost.
Classic pathology studies suggest that, by the time the typical motor symptoms of Parkinson’s appear, around 50%–70% of dopaminergic neurons are already lost from the brain. Similarly, in early clinical Alzheimer’s disease, where those affected have mild dementia, hippocampal volume in the brain seen on imaging is already up to 25% lower than that of age-matched controls. This means, however good the treatment is, the patients will never regain complete function.
“There’s no way we can restore these neurons,” said Roman Kniazev, CEO of U.S.-biotech Nuravax, which is developing several different Alzheimer’s vaccines. “They are gone forever. So that is why the best strategy, and this is our motto in our company, is to not let the pathology kill the neurons.”
Researchers trying to develop new therapies for Alzheimer’s and Parkinson’s are increasingly moving towards an early or even preventive approach. The idea of a vaccine-like approach to targeting Alzheimer’s is not new. Animal work in the late 1990s showed that vaccinating against amyloid‑beta could clear plaques and improve cognition in transgenic mouse models. This led to the development of Elan/Wyeth’s amyloid‑beta vaccine, AN1792.
It entered Phase I/II trials for mild‑to‑moderate Alzheimer’s and successfully induced anti‑amyloid beta antibodies in some patients. But the study had to be stopped in 2002 because around six percent of the participants developed meningoencephalitis, linked to T cell–mediated inflammation in the brain. Despite strong amyloid plaque clearance, there was little impact on symptoms in the clinical trial participants.
Several other candidates, designed to avoid the T-cell activation seen with AN1792, have been unsuccessfully trialed over the last two decades. Although largely safe and antibody-producing, most of these programs were discontinued due to a lack of efficacy.
The field has persevered despite this, with improvements in technology, safety, biomarkers, and clinical trial design having led to a new generation of vaccine candidates that, while not yet approved, are showing good results in Phase I and II trials.
Neil Warma CEO, ProMIS Neurosciences
“I think what we’ve learned over the past five or 10 years from other vaccine approaches is that the next generation are those that come with a very precise approach to generating antibodies against the toxic species of a given protein for that specific neurodegenerative disease,” said Neil Warma, CEO of ProMIS Neurosciences, a U.S.-based company taking an antibody and a vaccine-based approach to treating Alzheimer’s and other neurodegenerative diseases.
“Those are really the things that make the vaccine approach much more interesting now. The sophistication of the biomarkers, the data we’ve learned from past and current products in the market, and then this ability to design and create antibodies that are highly specific to a targeted pathogenic form of the protein.”
AC Immune has three active immunotherapy candidates in Phase II: an anti-amyloid beta therapy, ACI-24, that is being developed with Takeda; an anti-tau therapy, ACF 35, being developed with Johnson & Johnson; and an anti-alpha synuclein candidate targeting Parkinson’s disease.
Staining of neurons in the brain from Neil Cashman’s lab-1.
The company reported good results for its Parkinson’s Phase II study at the end of last year. The interim study results showed a 100% response rate and a good safety profile in people with early Parkinson’s disease. Alpha-synuclein and neurofilament light levels in the blood, as well as scores from standard movement tests, suggested that disease stabilization had occurred.
If confirmed by results from the second part of the study, this would be the first time that disease modification, rather than symptom management, has shown promise for Parkinson’s disease. It would also confirm alpha synuclein as a pathogenic contributor to the condition.
“The statistical variability was very, very small, which was a surprise to us. Every single marker, preclinical biomarker, clinical imaging, went into the same direction,” said Pfeifer. “For me, what was particularly rewarding was that there was a connection between the titers, so the antibody response in the people versus the reduction of this pathology … the alpha-synuclein versus the imaging, which showed that the neurons can be protected.”
Better targeting to improve safety and efficacy
A common theme among vaccine developers in the neurodegeneration space is precision targeting. There is a strong consensus that a lack of specificity when picking targets is likely why many trials failed to show efficacy and had significant side effect issues in the past.
Different companies or research groups back slightly different protein targets, but the experts all emphasize the importance of avoiding binding to inert plaque in the brain in Alzheimer’s disease, and of targeting toxic, misfolded proteins that are disease-specific.
“We provide the body with active immunotherapy, and then the body induces the antibodies. But what is important is that these antibodies are really specific for the pathological form,” said Pfeifer.
AC Immune is not the only company with a keen focus on tightening up targeting in this area. Alzinova is specifically targeting toxic amyloid beta oligomers with its lead candidate ALZ-101, a therapeutic Alzheimer’s vaccine.
It received a recent FDA Fast Track designation for ALZ-101 after good safety and efficacy data were reported last year from its completed Phase Ib clinical trial.
“They have shown in many in vitro and in vivo models that … when you remove these toxic oligomers using antibodies towards them, you can basically neutralize the toxicity in these extracts towards the neurons,” explained Labuda.
He added that many of the “vaccines, as well as the monoclonal antibodies, are going for the N-terminal part of the protein. … By doing that, you will target the monomers, all the fibrils, but most importantly, also the plaques. Very little will be left to bind to something else that might be more important for the disease. I think this is what we see with the current treatments on the market. There’s a lot of off-target effects … and that’s why we have these huge challenges.”
ProMIS is also targeting amyloid beta oligomers in Alzheimer’s using both a monoclonal antibody and vaccine approach. It has developed a special method with the help of artificial intelligence to develop antibodies, taking both conformational shape and protein sequence into account.
“These three-dimensional shapes don’t exist on monomers, and they’re buried in plaque. We’ve tried and tried and tried to get these antibodies to bind monomers, to bind plaque, and they really don’t, which is good,” said Warma.
“We’ve done side-by-side testing with other antibodies to see if ours is truly differentiated. … In many different studies before we got to the clinic, PMN-310, our therapeutic antibody, was the only one that bound oligomers and avoided monomers and plaque. All the others cross-reacted with everything.”
ProMIS is testing its PMN-310 antibody before moving on to the vaccine approach. “If we can come with that one-two punch to say we’ve got a drug now that can treat patients with Alzheimer’s, we’ve got the ability to detect the onset of disease pathology in Alzheimer’s, and we have a vaccine that prevents you from developing that disease, I mean, that would be a pretty powerful combination,” noted Warma.
Nuravax is aiming to address two key shortcomings of first‑generation Alzheimer’s vaccines, such as AN1792: the risk of problematic T cell-driven inflammation and uneven immune responses in older adults. Its MultiTEP‑based candidates (AV‑1959R, AV‑1980R, and Duvax) are engineered to elicit a strong, antibody‑dominant response against amyloid‑beta and tau while minimizing activation of potentially autoreactive T cells and maintaining effectiveness.
“The platform which we developed makes the vaccine highly immunogenic, and this high immunogenic feature is essential for diseases in the brain,” said Kniazev.
Kiran Bhaskar, PhD Professor University of New Mexico
Kiran Bhaskar, PhD, is a professor and group leader at the University of New Mexico. He has worked on Alzheimer’s disease for many years and is also a scientific co-founder of TheraVac Biologics. He and his colleagues are developing an anti-tau Alzheimer’s vaccine that is about to start human trials.
They are also aiming to reduce risks associated with immune reactions to vaccine adjuvants, which can contribute to ARIA, and have created a vaccine that does not need an adjuvant.
“We use a strategy called a virus-like particle,” he explained. “You don’t need to expect any side effects because of adjuvants. In this way, we trick the immune system into thinking that there is a viral attack on the body. It immediately starts an immune response against the virus-like particle and also anything sticking to the surface of those virus-like particles, which in this case is pathological or phosphorylated tau proteins.”
Overall, in the trials carried out so far in the active immune therapy space in Alzheimer’s disease, rates of ARIA have been very low, which is another selling point for the vaccine approach. “We don’t expect to see ARIA in active immunotherapy because we are using the host’s own immune response system to generate antibodies. … So that way there’ll be less unanticipated immune response,” explained Bhaskar.
Credit: Ake Ngiamsanguan / iStock / Getty Images Plus
Overcoming challenges on the road to the clinic
There is no doubt that active immunotherapies or vaccines to target Alzheimer’s and Parkinson’s disease are more advanced than they have ever been before, but they are still a long way from a mainstream rollout.
One reason the conversation has shifted is that the approval and broader use of the first anti-amyloid antibodies, for all their modest effect sizes and ARIA issues, shows that lowering the right protein species can slow deterioration. Using a more vaccine-like approach, where people make their own antibodies, does have the potential to make targeting these conditions safer, cheaper, and more accessible for patients.
But basic clinical questions remain unanswered. For example, how long vaccine-induced protection will last, how often boosters will be needed, and whether early stabilization of biomarkers and motor or cognitive scores—such as AC Immune’s interim Parkinson’s data or Alzinova’s Phase Ib Alzheimer’s study results—will translate into true preserved function a decade later.
Biomarkers are a big potential stumbling block for the development of preventive vaccines. The position is better for Alzheimer’s disease; the FDA’s approval of two blood-based Alzheimer’s biomarkers now gives developers a way to find people with silent pathologies without relying solely on positron emission tomography imaging. But there is still a lot more to do on this front, particularly in diseases like Parkinson’s, ALS, or other neurological or neurodegenerative diseases where less is known.
Credit: Martin Philip / iStock / Getty Images Plus
“We need better and safer treatments, but it’s also linked to having the right biomarkers, because if you have a risk factor, it doesn’t mean necessarily that you have the disease,” said Pfeifer. “These biomarkers are still not very well established. … The goal is absolutely to go to preclinical, and preclinical will require these biomarkers. If you ask me what is needed most in Parkinson’s right now, [it] is definitely to have better biomarkers.”
A second stumbling block for companies that want to develop vaccines that can effectively immunize people against neurodegenerative disease is that clinical trials of vaccines in populations of people with no symptoms have historically been large, expensive, and time-consuming—something out of reach of most biotechs without significant outside investment.
ProMIS and others are hoping that the efficacy of their therapeutic antibodies will boost their vaccine pipeline in the future. “If we show that it works in Alzheimer’s, then a similar approach should work in these other diseases,” said Warma. “Since it’s an almost identical process for vaccines, it also shows proof of concept for this whole wave of vaccines coming behind it.”
For now, active immunotherapies promise something that is more modest than true disease prevention but still crucially important. Namely, cheaper, less burdensome, and potentially safer ways to target the same disease biology as today’s monoclonal antibodies, ideally years earlier in the process.


 , is a blood-based test that assesses the immune and broader, relevant biological status of kidney transplant patients to identify the risk of all forms of acute rejection, including T cell (TCMR) and antibody-mediated rejection (ABMR). Tutivia combines transcriptomics with proprietary AI models to address this precise unmet need: biologically accurate insight into what is actually happening within the graft.
, is a blood-based test that assesses the immune and broader, relevant biological status of kidney transplant patients to identify the risk of all forms of acute rejection, including T cell (TCMR) and antibody-mediated rejection (ABMR). Tutivia combines transcriptomics with proprietary AI models to address this precise unmet need: biologically accurate insight into what is actually happening within the graft.